(UroToday.com) The 2024 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Emily Smyth discussing real-world treatment sequences and time to discontinuation in the first-line metastatic castration-resistant prostate cancer (mCRPC) setting. Despite treatment advances for metastatic prostate cancer, the average life expectancy is limited to 2-3 years following the development of mCRPC. In mCRPC, one of the main considerations for treatment selection is therapy received in prior settings, mainly metastatic hormone-sensitive prostate cancer (mHSPC). There is limited real-world data on treatment sequencing in metastatic prostate cancer. Additionally, while guidelines support adding novel hormonal agents to ADT for mHSPC, use is limited because of clinical and/or patient-driven factors. Dr. Smyth and colleagues evaluated treatment patterns, real-world time to discontinuation, and real-world time to chemotherapy for first-line mCRPC patients, including Black/African Americans, treated predominantly in a community oncology setting. Additionally, they analyzed systemic treatments before first-line mCRPC as well as progression to second-line mCRPC.
This retrospective study included patients with mCRPC from the nationwide Flatiron Health EHR-derived, deidentified database who initiated first-line treatment between January 2013 and January 2023, with a study end of April 2023. Treatment patterns were described by time period of first line initiation: time period 1 – January 2013 – December 2017 and time period 2 – January 2018 – January 2023:

Kaplan-Meier analyses were conducted for real-world time to discontinuation/time to chemotherapy, and a Cox proportional hazards regression model was used to determine the association between patient characteristics and real-world time to discontinuation/time to chemotherapy for first line mCRPC. Subgroup analyses were performed for Black/African Americans.
Among the 8,915 first line-treatment patients with a median age of 74 years, and 871 (10%) men were Black/African Americans (median age 70 years):
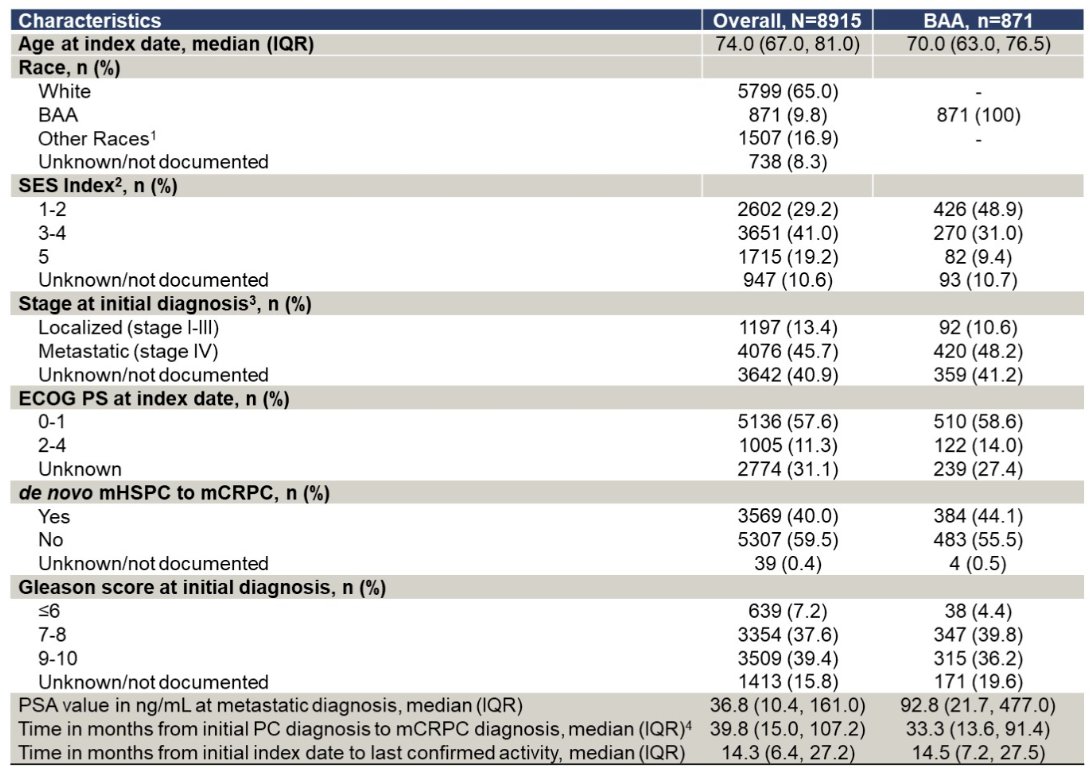
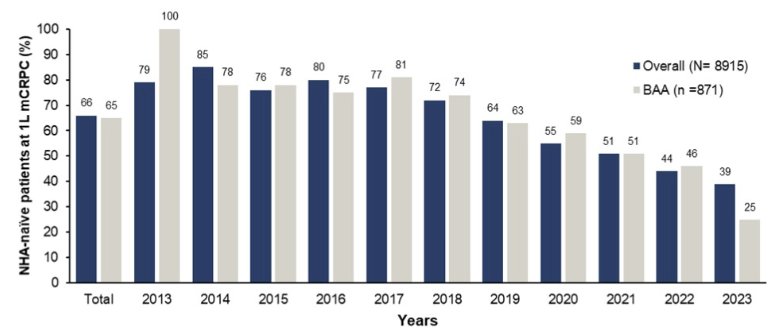
There were 5,870 (66%) men on novel hormonal agents-naïve at first-line mCRPC, including 65% of the Black/African American cohort. Overall, the percent of patients who were on novel hormonal agent-naïve treatment decreased from 2018 (72%) to 2023 (39%) and a similar trend was observed for Black/African Americans (74% [2018] to 25% [2023]):
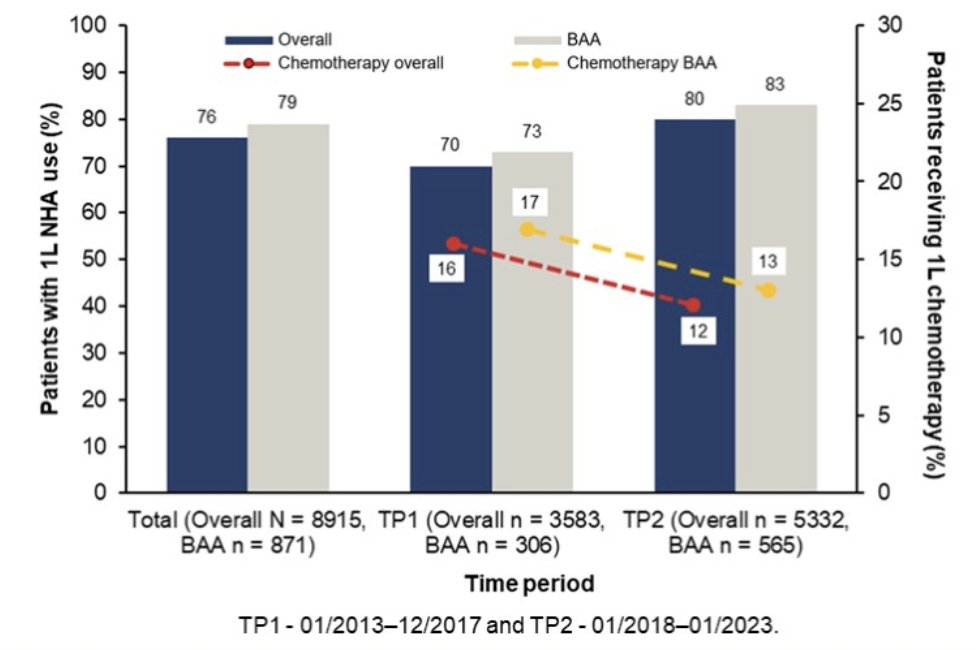
First-line novel hormonal agents use in mCRPC increased from time period 1 to time period 2 (overall: 70% to 80%; Black/African Americans: 73% to 83%), primarily driven by enzalutamide (overall: 30% to 39%; Black/African Americans: 33% to 38%) and decrease in chemotherapy (overall: 16% to 12%; Black/African Americans: 17% to 13%). The top three first line mCRPC regimens for the overall population and Black/African Americans were abiraterone (35%; 38%), enzalutamide (32%; 33%), and docetaxel (10%; 11%):
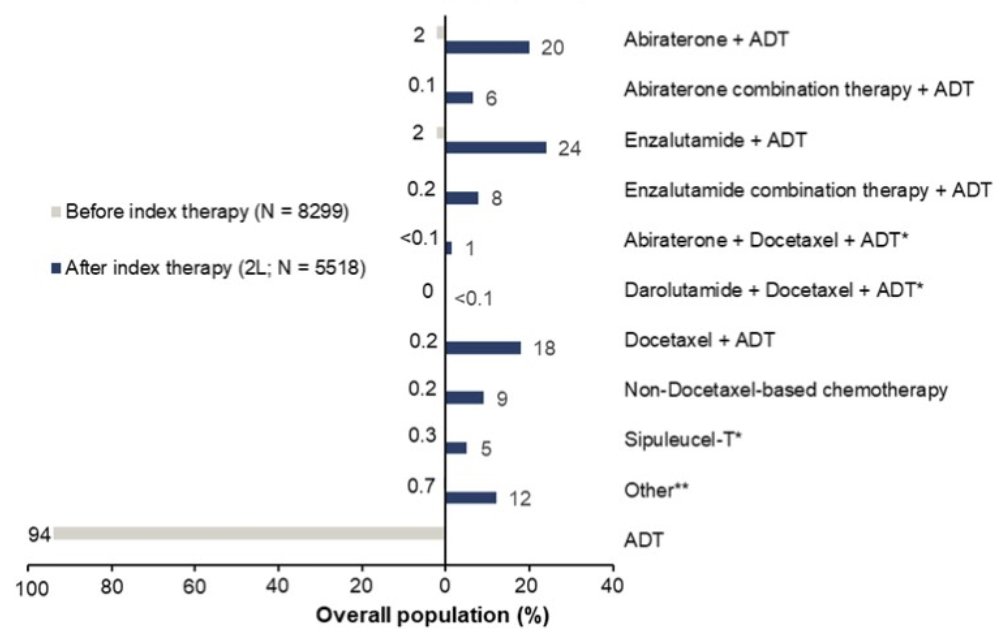
Among patients who progressed to second-line mCRPC, the most common sequences for patient treatment with abiraterone or enzalutamide for first-line mCRPC were ADT monotherapy in the prior line of treatment and a switch to abiraterone (20%) or enzalutamide (24%) upon progression from first line to second line:
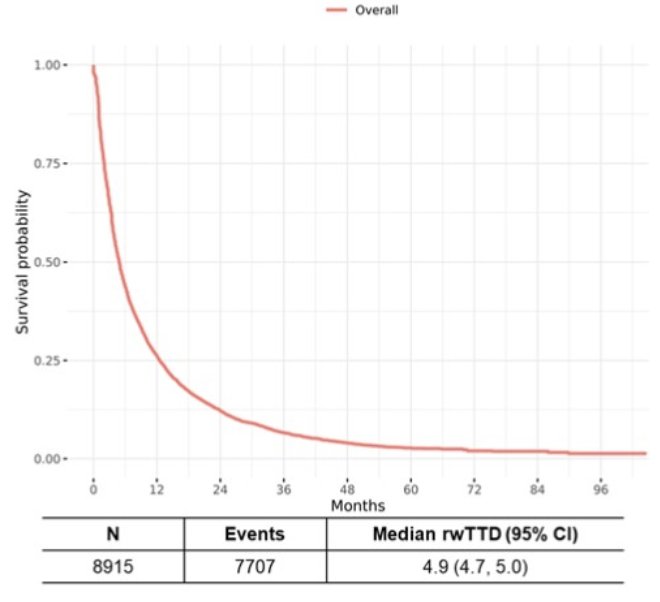
In the overall population, real-world time to discontinuation was a median 4.9 months (95% CI 4.7 – 5.0):
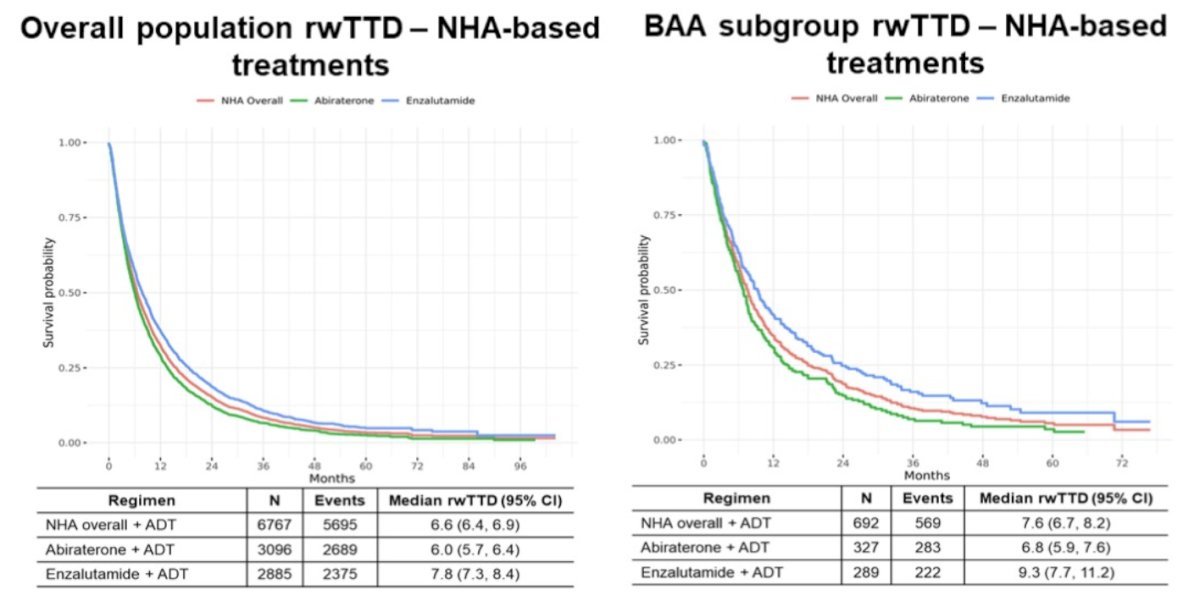
The overall population and Black/African American real-world time to discontinuation among novel hormonal-based treatments is as follows:
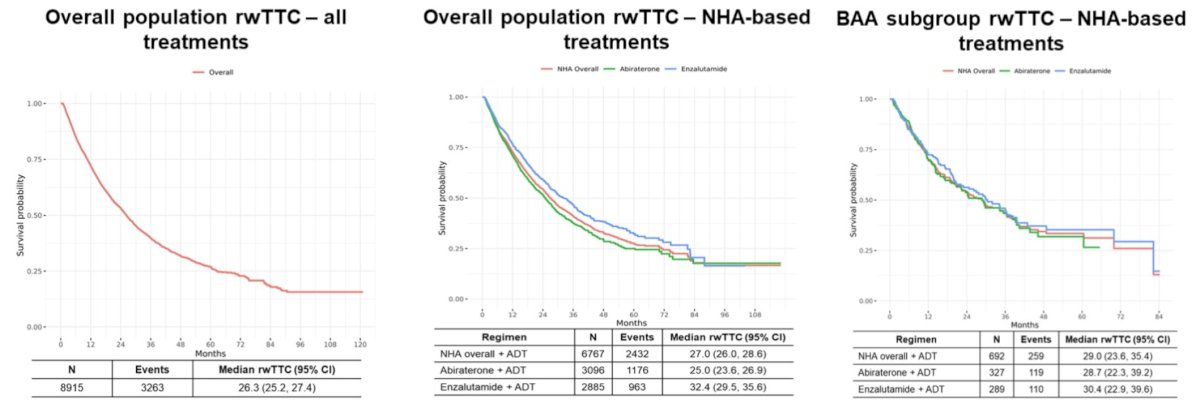
Age ≥ 80 years, ECOG performance ≥1, socioeconomic status = 5 (highest), and median time ≤ 39.8 months from initial diagnosis to mCRPC were associated with a higher hazard of discontinuation (all p ≤ 0.05). Finally, the following figures highlight real-world time to chemotherapy:
Dr. Smyth concluded her presentation discussing real-world treatment sequences and time to discontinuation in the first-line mCRPC setting with the following take-home points:
- Overall, most patients received their first novel hormonal agents in first line mCRPC, however there was an increase novel hormonal agent utilization at first line mHSPC treatment following approval in this setting
- Novel hormonal agents use increased and chemotherapy use decreased from time period 1 to time period 2
- There was heterogeneity in treatment sequences in patients treated with a novel hormonal agent in first line mCRPC, with some patients treated with an alternative novel hormonal agent in the second line despite a lack of robust evidence to support this
- Nearly 50% of Black/African American patients and 30% in the overall cohort had an SES score of 1-2, indicative of low socioeconomic status. The clinical implications of socioeconomic status and potential impact on treatment outcomes should be considered
- Overall, first line real-world time to discontinuation was short with a small numerical increase in time period 2
- Factors contributing to discontinuation, such as treatment resistance, need to be better understood to further improve real-world outcomes
Presented by: Emily Nash Smyth, PharmD, BSPharm, Eli Lilly and Company, Indianapolis, IN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, San Francisco, CA, January 25th – January 27th, 2024