(UroToday.com) The 2024 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Petros Grivas discussing results from the real-world US PATRIOT-II study assessing avelumab first-line maintenance therapy for locally advanced/metastatic urothelial carcinoma. Urothelial carcinoma accounts for approximately 90% of all bladder cancer, with a 5-year survival rate of 38% for locally advanced disease and 5% for metastatic disease. Platinum based chemotherapy is a standard of care for first line treatment for eligible patients with locally advanced/metastatic disease, however despite high initial response rates, durable responses are uncommon, and most patients ultimately experience disease progression in a median of ~9 months after the start of treatment. In the JAVELIN Bladder 100 phase 3 trial, avelumab first-line maintenance + best supportive care improved overall survival and progression-free survival vs best supportive care alone in patients with locally advanced/metastatic urothelial carcinoma with no disease progression following 4-6 cycles of platinum-based chemotherapy.1 PATRIOT-II aimed to describe real-world outcomes in patients with locally advanced/metastatic urothelial carcinoma treated with avelumab first-line maintenance who were progression-free after first line platinum-based chemotherapy. Dr. Grivas and colleagues hypothesized that outcomes would be similar to those of JAVELIN Bladder 100.
PATRIOT-II is an observational, retrospective study in US patients with locally advanced/metastatic urothelial carcinoma treated in 37 geographically dispersed community and academic centers:
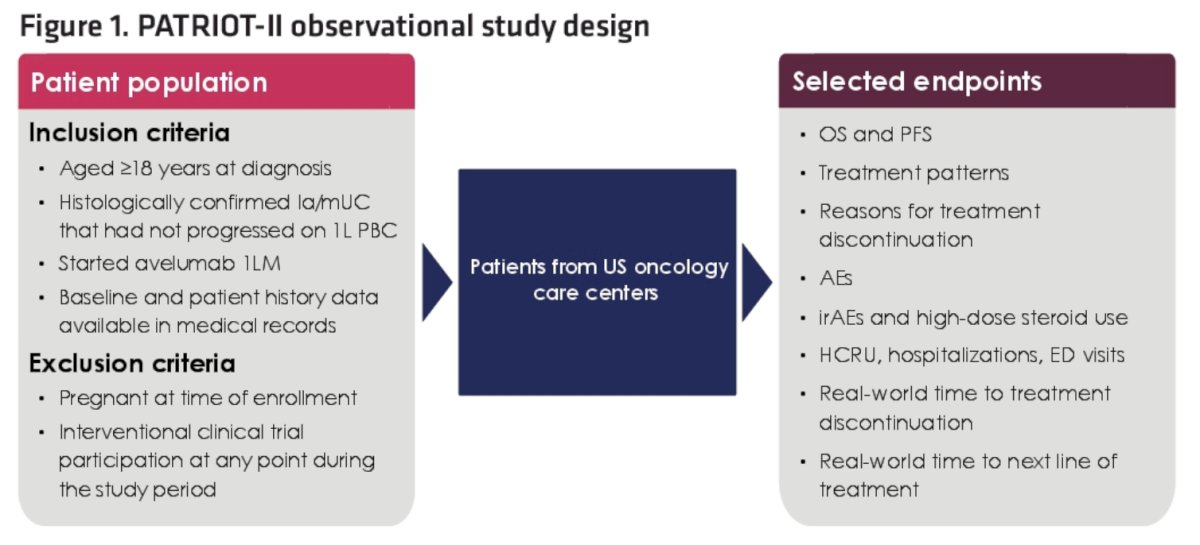
Patients receiving avelumab first-line maintenance were eligible, and data were collected via medical records for a minimum of 52 weeks from avelumab first-line maintenance initiation. This analysis focuses on ≥24 weeks post avelumab first-line maintenance initiation. Survival and safety outcomes were assessed and analyses are descriptive in nature. Time to event outcomes were examined using the Kaplan Meier analysis and life tables, censoring for the end of study or loss of follow-up in patients not meeting a terminal endpoint.
There were 160 patients from 37 sites, with a mix of oncology practices and community/academic centers. The median age was 70 years (range: 40-90), 123 (77%) patients were male, 118 (74%) were White, non-Hispanic, 77 (49%) had lower urinary tract disease and 49 (31%) upper tract tumors, 119 (74%) had a ECOG performance status 0/1, 70 (44%) and 51 (32%) had known visceral (excluding bone) or non-visceral metastases, respectively, 31 (19%) had liver mets, and 64 (40%) had a creatinine clearance >60 mL/min. There were 100 (62.5%) patients and 60 (37.5%) patients that received first line cisplatin or carboplatin, respectively:
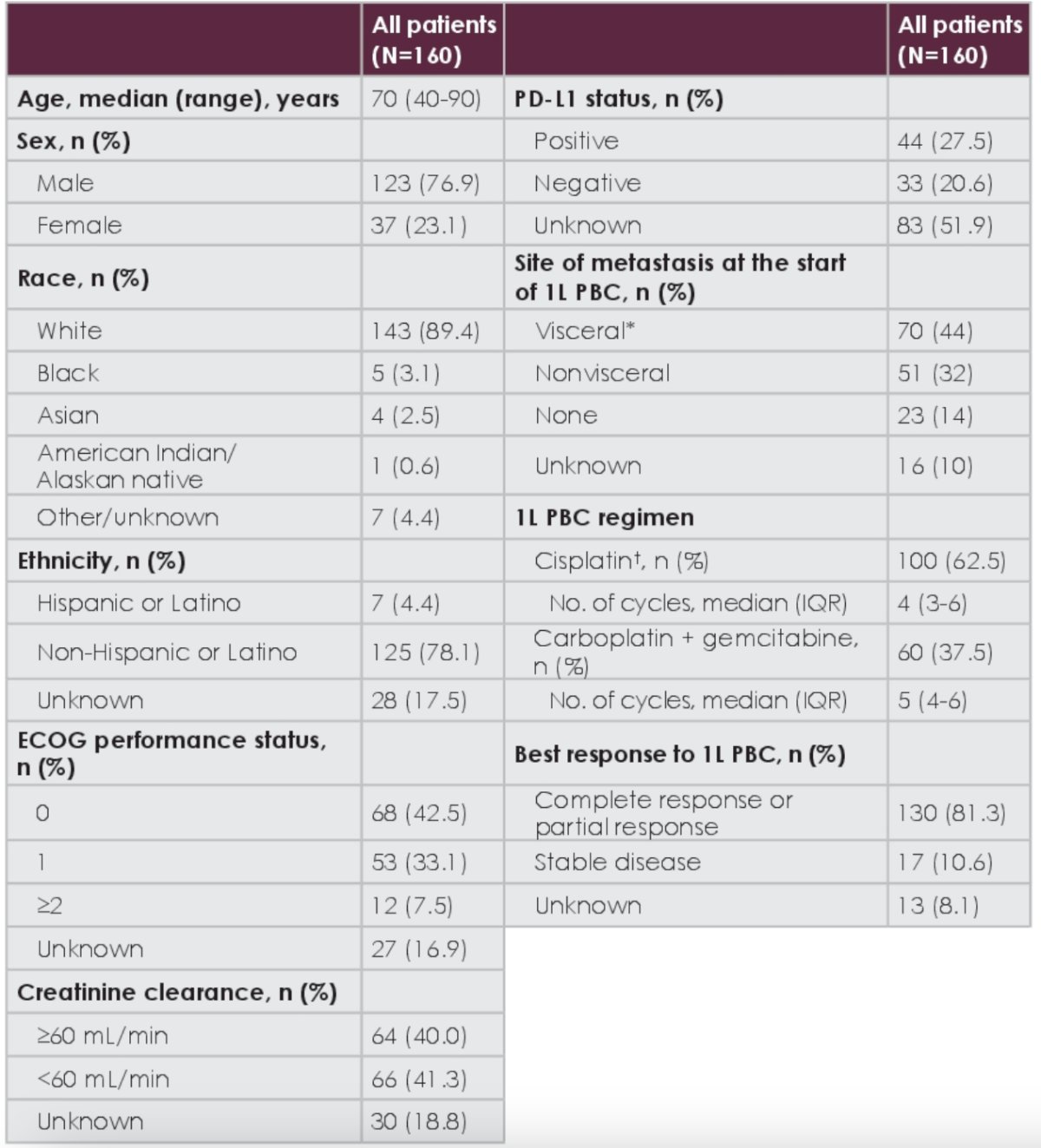
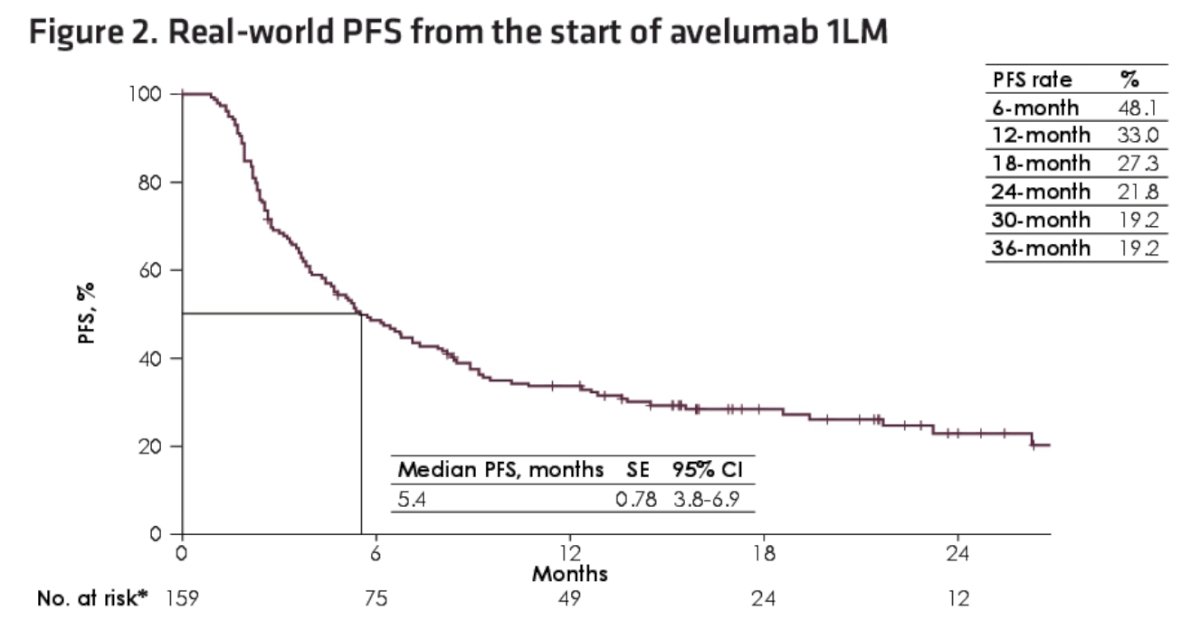
Overall, 130 patients (objective response rate: 81% [complete response: 21, 13%; partial response: 109, 68%]) had an investigator-assessed response to first line platinum-based chemotherapy. The patients initiated avelumab first-line maintenance at a median of 4 weeks (IQR 3-6) after platinum-based chemotherapy completion. At the time of data cutoff, 31 patients (19%) continued to receive avelumab treatment, and 118 patients (74%) had discontinued avelumab first-line maintenance due to progression/adverse events/other non-death related reasons. The median time on avelumab first-line maintenance was 4.1 months (IQR 2.3-8.7), and the median follow-up time post avelumab first-line maintenance initiation was 16 months (IQR 11-21). The median real-world PFS from the start of avelumab was 5.4 months (95% CI 3.8-6.9):
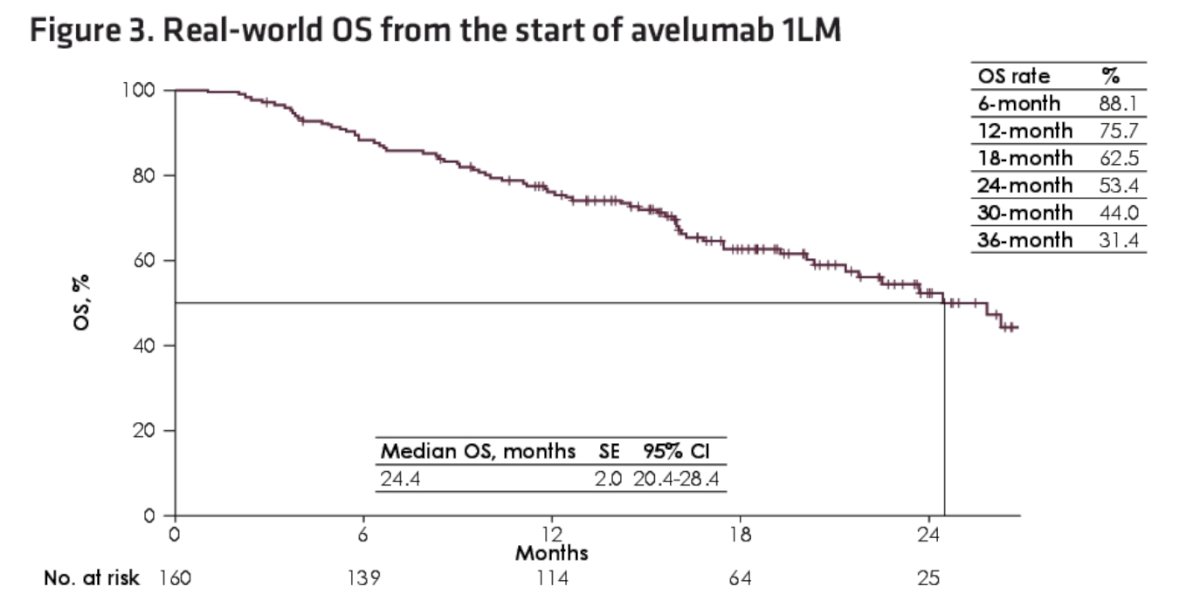
The median real-world overall survival was 24.4 months (95% CI 20.4-28.4):
In the patient cohort without disease progression after first line platinum based chemotherapy, the median real world overall survival from the start of first line chemotherapy was 30.5 months (95% CI 23.4-37.6):

Overall, 62 patients (39%) had an adverse event related to avelumab and 35 patients (22%) had an immune-related adverse event. The most common documented treatment-related adverse events (any grade) included hypothyroidism (n=7 [4%]), anemia (n=6 [4%]), creatinine increase (n=6 [4%]), fatigue (n=6 [4%]), and nausea (n=6 [4%]). Grade 3+ adverse events occurred in 19 (12%) patients, with no Grade 5 adverse events.
During the avelumab treatment period, 44 patients (28%) were hospitalized for a mean of 11.5 days per person-year, with avelumab-related adverse events being the reason for admission in 13 patients (8%), and the remainder secondary to disease progression, surgical procedures, and comorbidities:

Several limitations of the study include the retrospective data, lack of randomization and central scan review, missing data, selection bias, and confounders.
Dr. Grivas concluded his presentation by discussing results from the real-world US PATRIOT-II study assessing avelumab first-line maintenance therapy for locally advanced/metastatic urothelial carcinoma with the following take-home points:
- Real world overall survival and progression free survival results in PATRIOT-II are in line with findings from the JAVELIN Bladder 100 trial, with no new safety concerns
- This real world study further supports the level I evidence for avelumab first-line maintenance as standard of care in locally advanced/metastatic urothelial carcinoma not progressing on first line platinum-based chemotherapy
Presented by: Petros Grivas, Division of Hematology & Oncology, University of Washington & Fred Hutchinson Cancer Center, Seattle, WA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, San Francisco, CA, January 25th – January 27th, 2024
References: