(UroToday.com) The 2024 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to a session on optimizing treatment strategies for patients with positive pelvic and/or retroperitoneal lymph nodes. In her presentation. Dr. Monika Joshi discussed:
- The role of systemic therapies in patients with lymph node positive, non-metastatic bladder cancer
- The role of systemic therapies in retroperitoneal nodal positive, M1a bladder cancer in those with a clinical complete response
- The role of biomarkers, such as circulating tumor DNA (ctDNA), in guiding treatment
Dr. Joshi emphasized that systemic disease mandates systemic therapy. N+ or M1a disease is a systemic disease state with distant micro-metastasis present, even if often not visible with conventional scans, and is associated with worse survival compared to localized disease. A clinical complete response is not durable after chemotherapy, with very short progression-free survival, with patients harboring node-positive disease having significantly worse survival outcomes.1
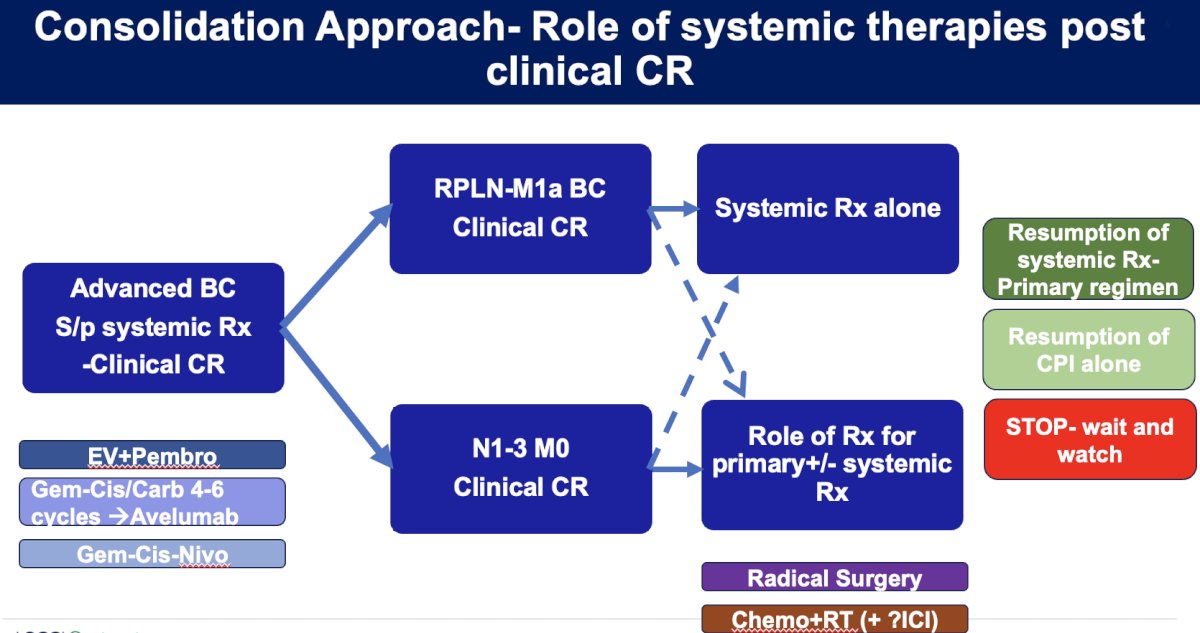
Dr. Joshi shared her current consolidation approach in patients with a clinical complete response post-systemic therapy. Current 1st line treatment options for patients with locally advanced/metastatic urothelial carcinoma include enfortumab + pembrolizumab, gemcitabine + cisplatin/carboplatin followed by maintenance avelumab, or nivolumab + gemcitabine/cisplatin. Dr. Joshi noted that among patients with retroperitoneal nodal positive (M1a) bladder cancer patients who achieve a clinical complete response, her preferred approach is to consolidate with systemic therapy alone. There may be a role for primary therapy, with or without additional systemic therapy; however, this approach is less preferred for such patients with advanced stage disease. Conversely, for those with N1-3M0 disease who achieve a complete clinical response, primary +/- systemic therapy may be strongly considered for select patients. This plot ‘thickens’ further following the consolidation therapy – should we stop therapy in these patients and ‘wait and watch’, should we resume systemic therapy, or resume a checkpoint inhibitor alone, for example?
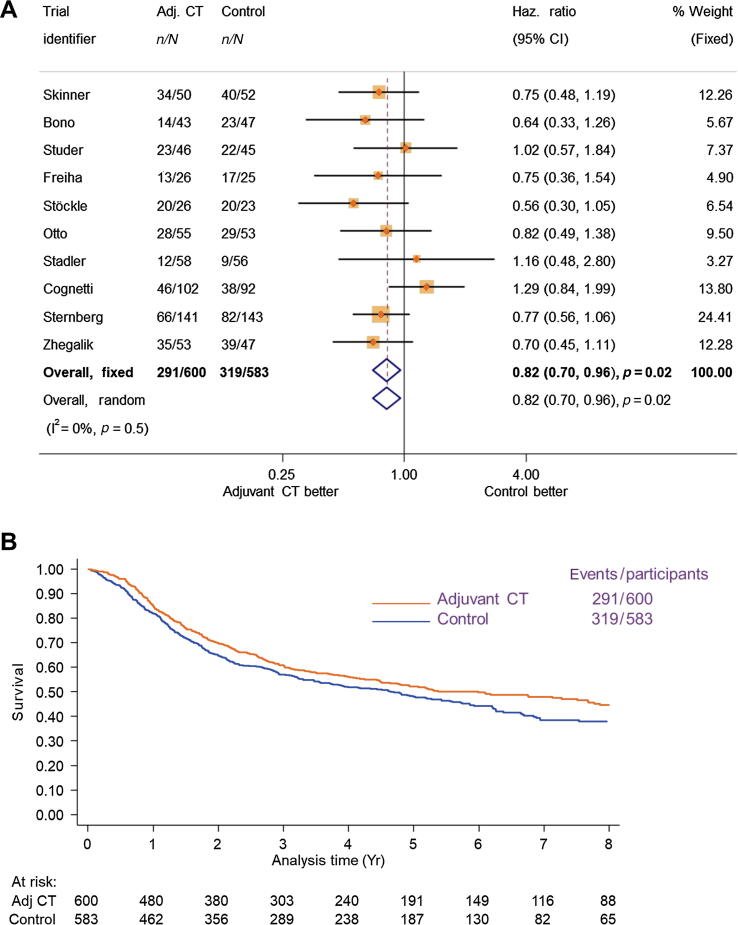
What is the current evidence for chemotherapy-based treatment in patients with node-positive, M0 disease? In the neoadjuvant setting, there is weak evidence for cisplatin-based chemotherapy. Most trials restricted the involvement of LN+ stage to cN1 (<2cm in most studies). There is a lack of phase 3 randomized controlled trials with neoadjuvant chemotherapy for those with cN+ disease. Conversely, in the post-radical cystectomy adjuvant setting, a 2022 Advanced Bladder Cancer individual participant data (IPD) meta-analysis of 10 RCTs (n=1,183) demonstrated that adjuvant cisplatin-based chemotherapy improved 5-year overall survival by 6% (HR: 0.82, p=0.02) for patients with muscle-invasive bladder cancer. There, however, was no clear benefit for patients with pN+ disease, with a HR of 1.44 (95% CI: 0.91 – 2.29) for pN1 patients and HR of 1.15 (95% CI: 0.73 – 1.80) for pN2 patients.2
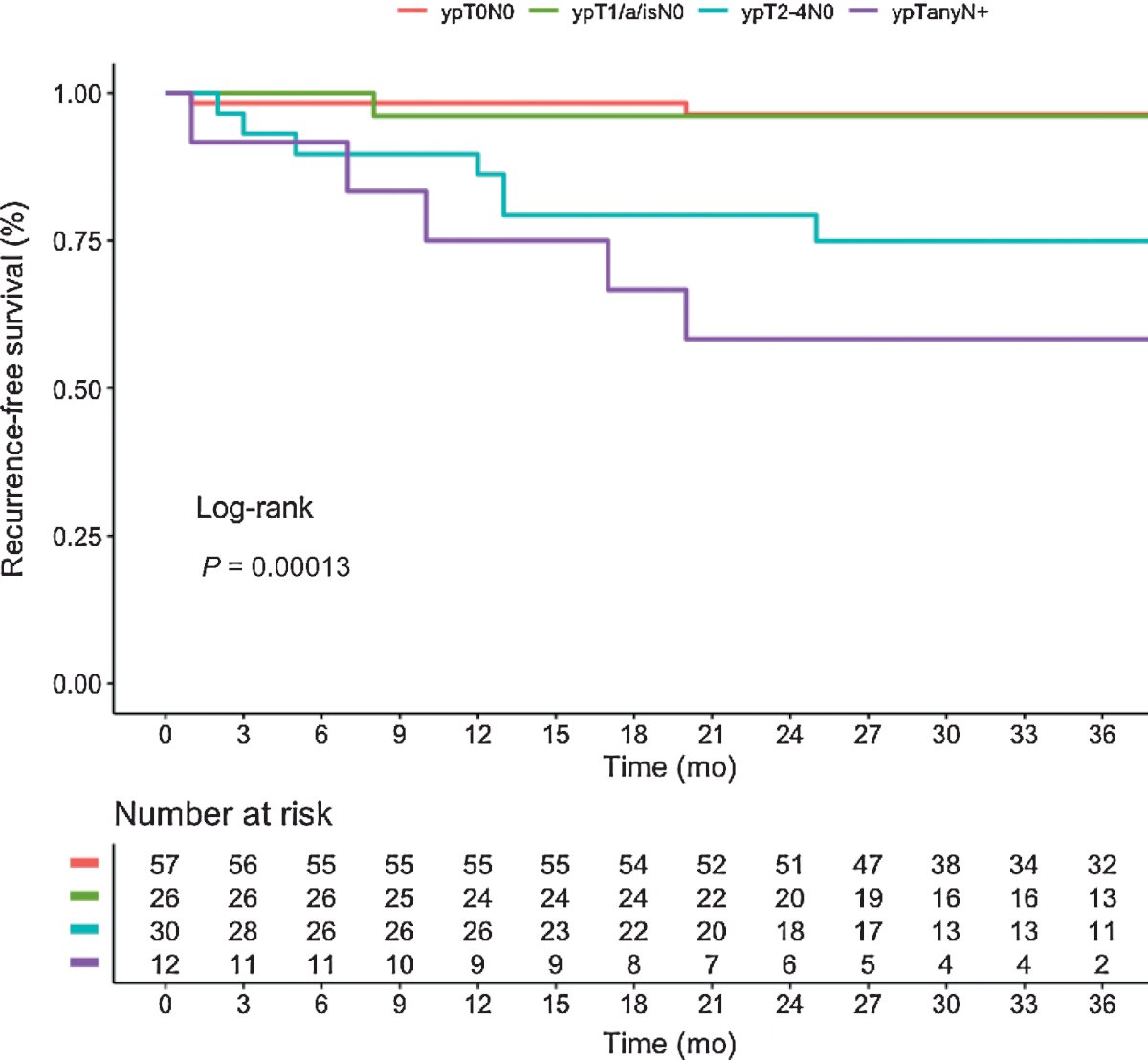
What about the use of checkpoint inhibitors for LN+ M0 patients? Similar to the neoadjuvant chemotherapy trials, neoadjuvant immune checkpoint inhibitor trials were mostly limited to patients with cN0 disease. In the PURE-01 trial of neoadjuvant pembrolizumab administered for three cycles in 155 patients with cT2-4N0 disease, the pathologic complete response (pCR) at radical cystectomy was 42%. 86.4% of patients received no further treatment following pembrolizumab, and 12 did not undergo a radical cystectomy. At a median follow-up of 39 months, the event-free and overall survivals were 75% and 84%, respectively. Dr. Joshi noted that patients with pN+ disease had significantly worse recurrence-free survival outcomes.3 Thus, although systemic therapy is the backbone treatment for such patients, it is clear that such patients fare worse compared to those with localized disease, even when systemic therapy is administered.
Similarly, the ABACUS trial of two cycles of neoadjuvant atezolizumab in 95 patients with cT2-4N0 muscle-invasive bladder cancer demonstrated a pCR of 31%, with 2-year disease-free and overall survival rates of 58% and 77%, respectively. Notably, ctDNA seemed to be prognostic biomarkers, with ctDNA+ patients benefiting more from systemic therapy in this setting.4 There are currently numerous ongoing phase 3 trials in this setting for patients with cT2-4aN0-1M0 or cT1-4aN1M0 disease, including VOLGA (NCT04960709), KEYNOTE-B15/EV-304 (NCT04700124), and KEYNOTE-905 (NCT03924895) EV+ CPI combination.
Conversely, in the adjuvant setting, there is evidence available for the use of adjuvant checkpoint inhibitor therapy post-radical cystectomy from trials such as CheckMate 274,5 IMvigor010,6 and AMBASSADOR, which is being presented at GU ASCO 2024 by Dr. Andrea Apolo, with these trials including patients with pN+ disease.

What about the evidence available for consolidation with multimodality approaches for LN+ M0 patients? In 2023, Dr. Joshi and colleagues published the results of DUART (BTCRC-GU15-023), which was a single-arm, multi-institutional phase II study of 26 patients with pure or mixed urothelial bladder cancer (T2-4N0-2M0) with unresectable tumors and who were unfit for surgery or cisplatin ineligible. Patients received durvalumab concurrently with radiotherapy for seven weeks, followed by adjuvant durvalumab for one year.
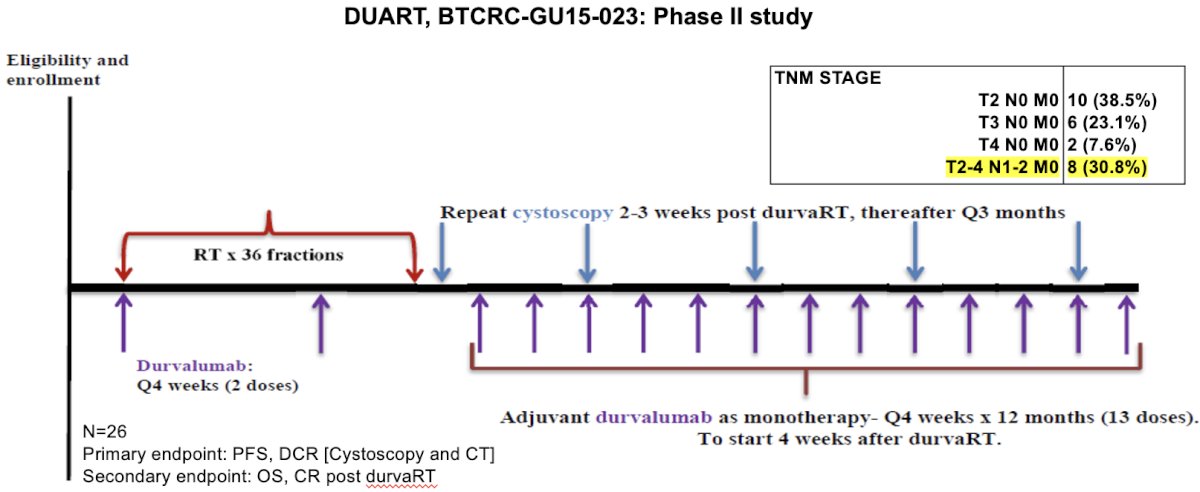
Although the sample size was small, there was evidence that survival outcomes were similar for MIBC patients, irrespective of their nodal positive status, when treated with durvalumab + radiotherapy followed by adjuvant durvalumab in the DUART study.7
- Progression-free survival (PFS) for LN+
- Median PFS 25.1 months
- 1-year PFS: 86%
- 2-year PFS: 57%
- OS for LN+
- Median OS: Not reached
- 1-year OS: 100%
- 2-year OS: 88%
- PFS and OS are better for those achieved CR/PR
- Median PFS: 31.7 months versus 7.9 months
- Median OS: 31.7 months versus 21.7 months
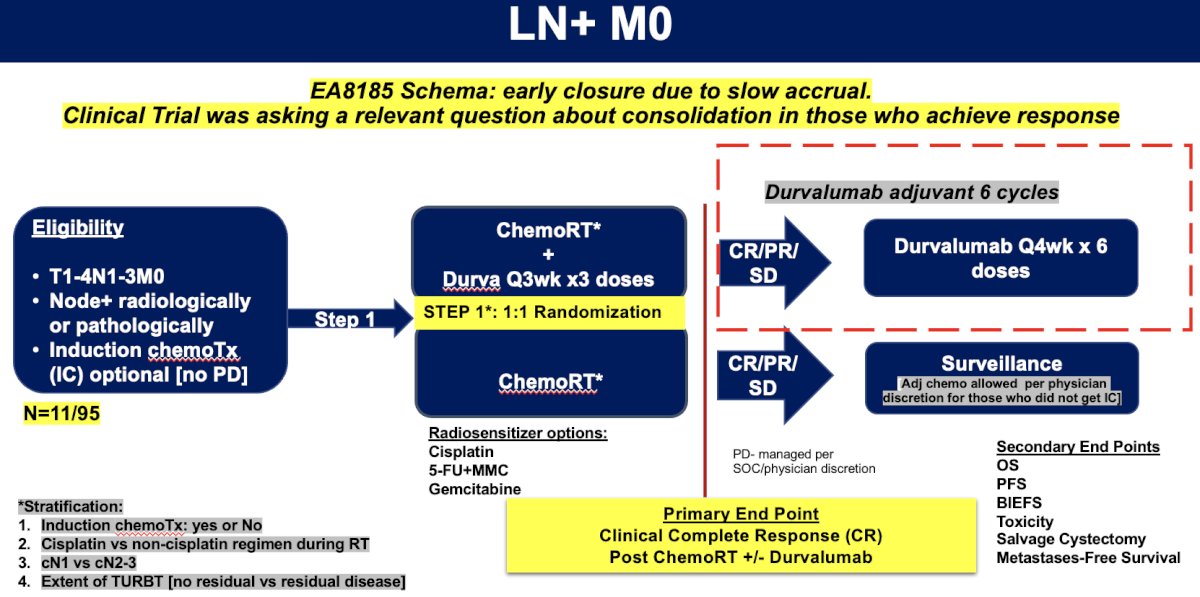
Dr. Joshi highlighted the study design for the EA8185 trial, which was closed early due to slow accrual. She noted that this trial was asking a relevant question about consolidation in those who achieve a response. Trial-eligible patients included those with T1-4N1-3M0 disease with node positive disease, either radiographically or pathologically, who were randomized 1:1 to chemoradiation +/- durvalumab. Among patients who have evidence of no disease progression (i.e., complete/partial response or stable disease), patients would have been randomized to durvalumab x 6 doses versus surveillance, with adjuvant chemotherapy allowed per physician discretion for those who did not receive immune checkpoint inhibitor therapy.
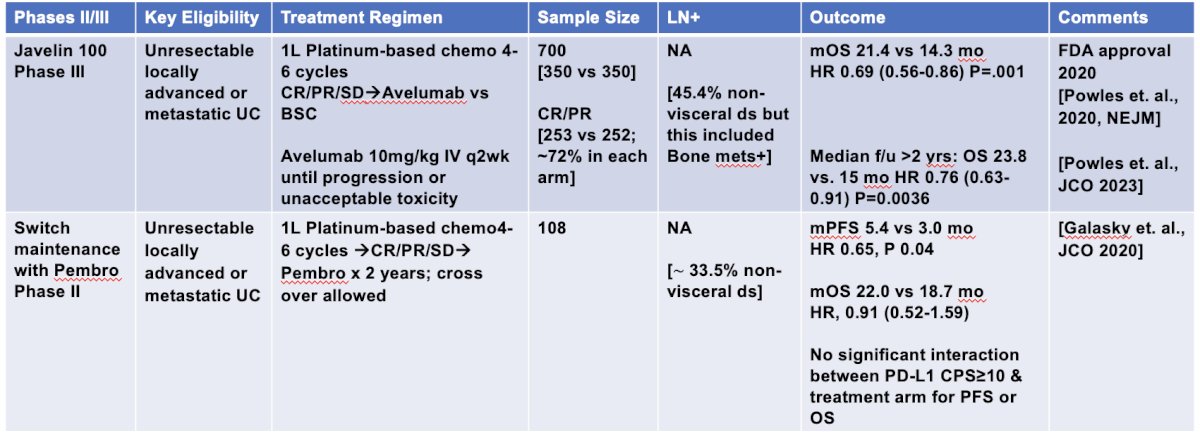
What about checkpoint inhibitor therapy for patients with evidence of retroperitoneal nodal positive disease (i.e. M1a)? There is level one evidence that maintenance checkpoint inhibitors (avelumab and pembrolizumab)8,9 provide an overall survival benefit in patients without evidence of disease progression following 1st line chemotherapy treatment.
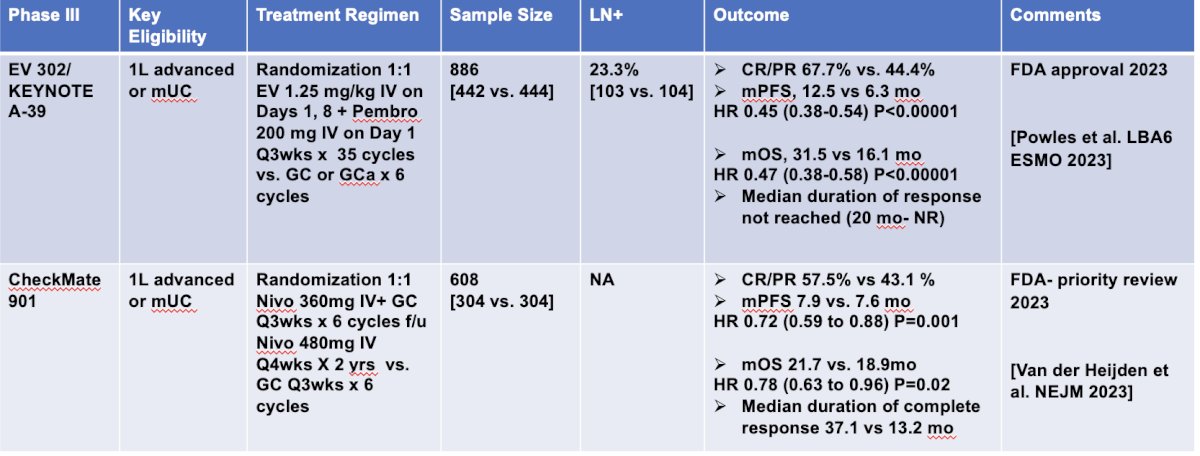
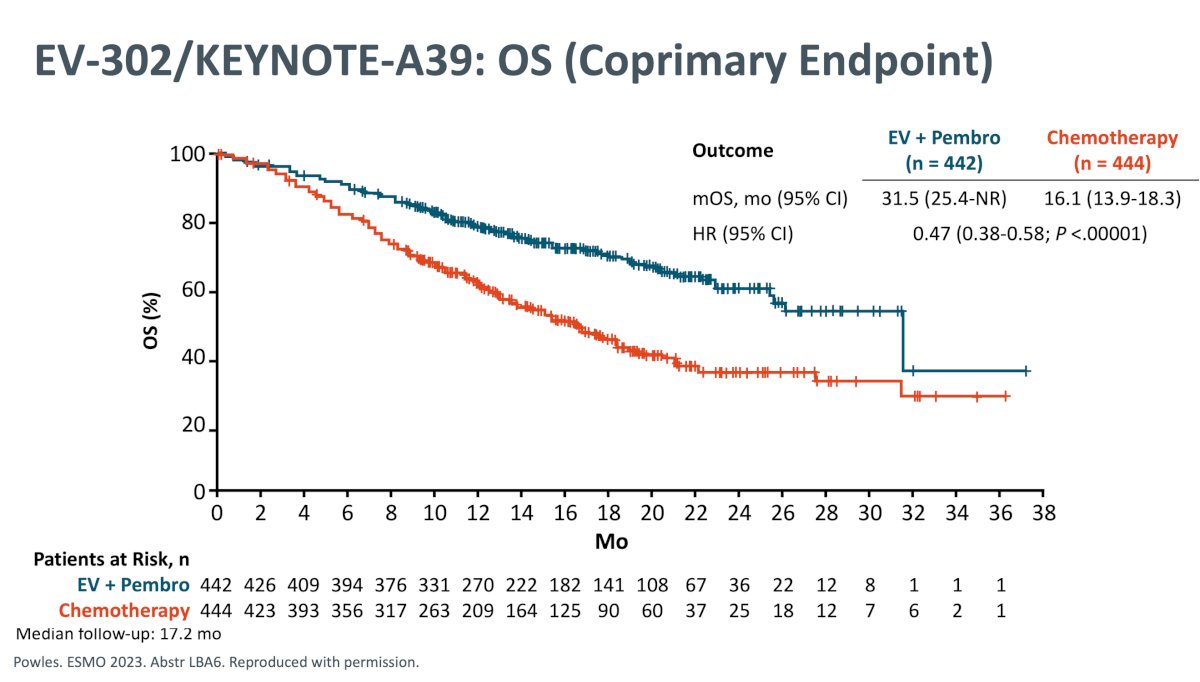
Dr. Joshi noted that with the emergence of novel 1st line combination approaches (enfortumab vedotin + pembrolizumab and nivolumab + gemcitabine/cisplatin10), such systemic treatment approaches may become standard of care systemic therapy for LN+ M0 bladder cancer patients. These trials, particularly EV-302/KEYNOTE-A39 with enfortumab vedotin + pembrolizumab, have raised the bar for systemic therapy options for LN+ or M1a urothelial carcinoma with a ‘new’ median overall survival of approximately 31 months, compared to the old reference of 16 months with cisplatin-based combination chemotherapy.
Given the multitude of treatment options available across the multiple treatment settings (i..e, neoadjuvant, 1st line systemic, adjuvant, maintenance, etc.), can we use biomarkers to guide treatment for metastatic urothelial carcinoma patients? Possible biomarkers include:
- PD-L1 status
- Tumor mutational burden (TMB) status
- ctDNA status
- Gene expression profile
- Presence/absence of DDR gene alterations
- Other next generation sequencing markers

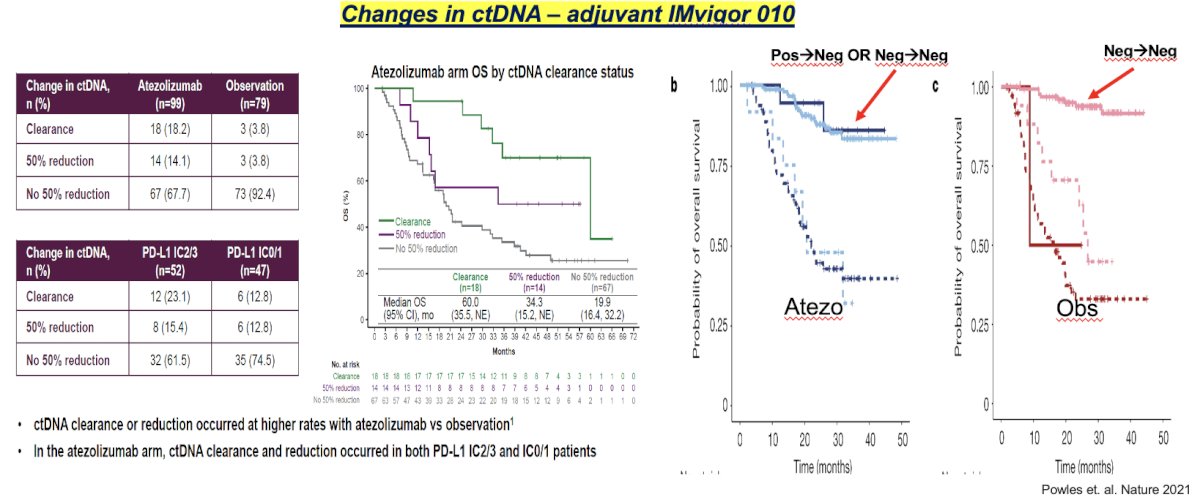
There is evidence from the IMvigor 010 trial of adjuvant atezolizumab that ctDNA may be both a predictive and prognostic biomarker in this setting, whereby ctDNA may act as a measure of minimal residual disease and an estimate of ‘molecular remission’. While IMvigor 010 was a negative trial that failed to meet its primary endpoint in the overall cohort, ctDNA+ patients who received atezolizumab had a significantly improved disease-free survival, compared to those who were observed (HR: 0.58, 95% CI: 0.43 to 0.79, p=0.0024). Conversely, ctDNA- patients receiving atezolizumab derived no survival benefit.6 Thus, ctDNA is a potential predictive biomarker in this setting.
Furthermore, it appears that ctDNA dynamics are of utmost prognostic significance in this adjuvant setting. ctDNA clearance or reduction occurred at higher rates with atezolizumab. Among patients in the atezolizumab arm, those who achieved ctDNA clearance had significantly improved overall survival compared to those with 50% or no reduction in ctDNA levels. Patients in the atezolizumab arm who cleared their ctDNA (i.e., positive to negative) had similar survival outcomes to those who were negative throughout, thus highlighting ctDNA as a promising prognostic biomarker in this setting.
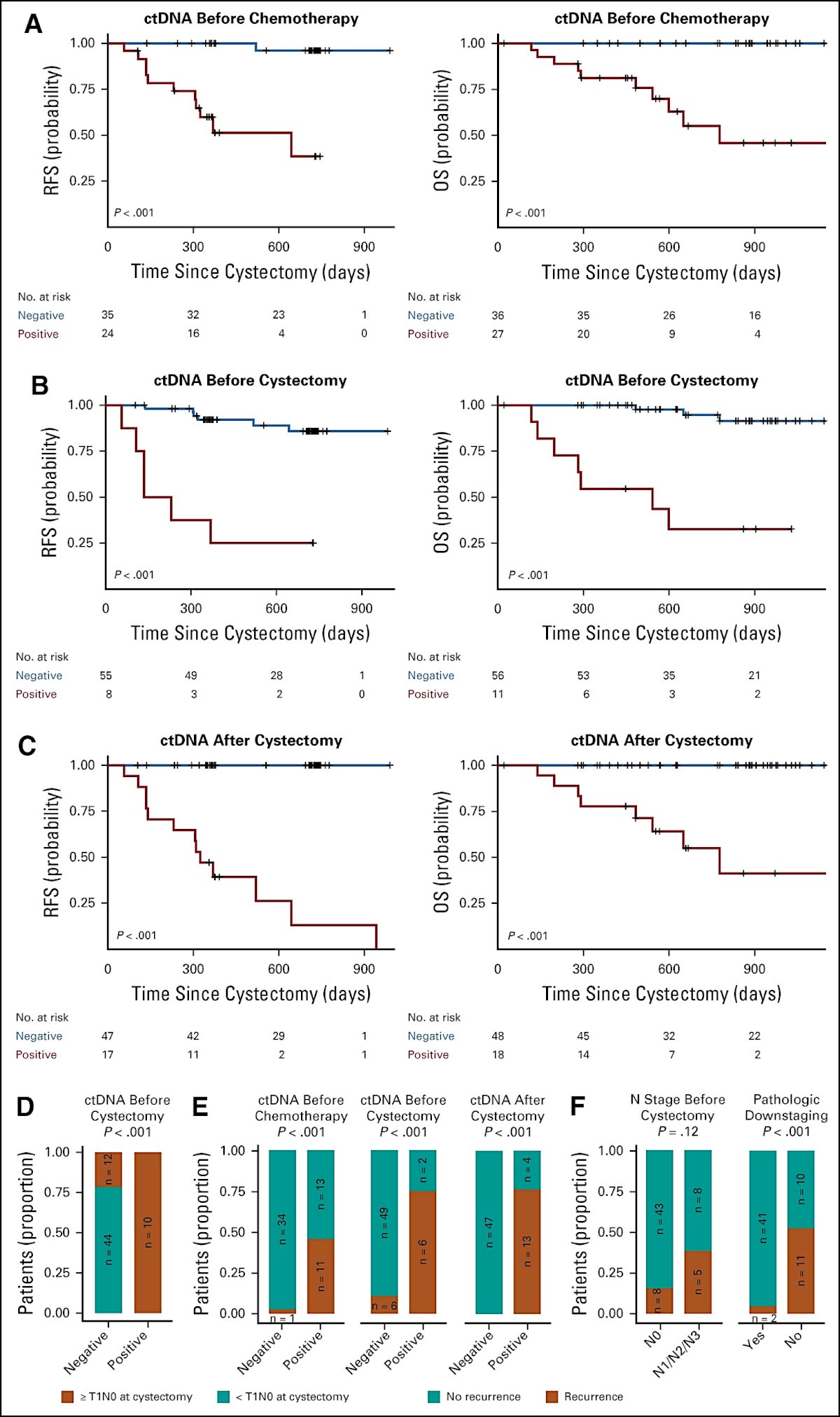
ctDNA may also be of excellent prognostic value in patients receiving neoadjuvant chemotherapy followed by radical cystectomy for muscle-invasive bladder cancer. In 2019, Christensen et al. published the results of an analysis of 68 patients with localized advanced bladder cancer. Patient-specific somatic mutations, identified by whole-exome sequencing, were used to assess ctDNA by ultra-deep sequencing of plasma DNA. Plasma samples (n = 656) were procured at diagnosis, during chemotherapy, before cystectomy, and during surveillance. Presence of ctDNA was highly prognostic at diagnosis before chemotherapy (HR: 29.1, p=0 .001). After cystectomy, ctDNA analysis correctly identified all patients with metastatic relapse during disease monitoring (100% sensitivity, 98% specificity). A median lead time over radiographic imaging of 96 days was observed. In addition, for high-risk patients (ctDNA positive before or during treatment), the dynamics of ctDNA during chemotherapy were associated with disease recurrence (p=0.023), whereas pathologic downstaging was not.11
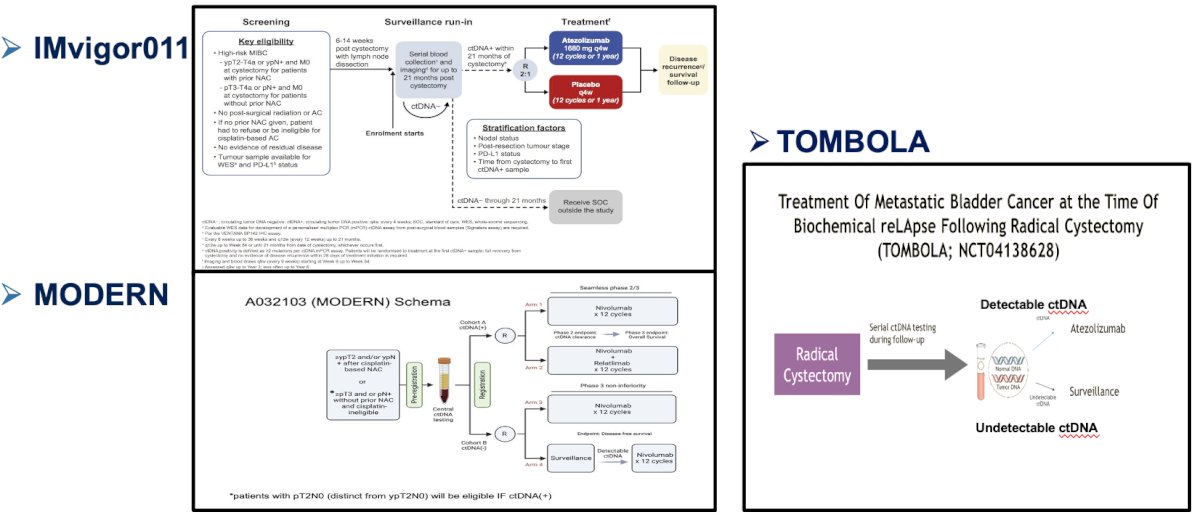
There are currently numerous ongoing studies of ctDNA-based treatment approaches, as summarized below:
Dr. Joshi argued that we need to adapt the use of prognostic/predictive biomarkers to the metastatic urothelial carcinoma setting to personalized treatment for complete clinical response with a negative ctDNA status, particularly when considering bladder preservation approaches. In such trials, treatment would be ‘escalated’ or ‘de-escalated’ depending on the biomarker status.
Dr. Joshi concluded her presentation as follows:
- Currently, there is no Level 1 evidence for consolidation in locally advanced LN+ or metastatic urothelial carcinoma with limited disease burden, such as cN+ or M1a who achieve clinical complete response
- Consideration of consolidation treatments for residual lesions such as stereotactic body radiotherapy +/- external beam radiotherapy/radical cystectomy to the primary to improve overall outcome in complete clinical responders seems reasonable: there is an urgent need for clinical trials
- NGS, TMB, PD-L1, etc. may have predictive or prognostic value.
- ctDNA (as a surrogate for minimal residual disease) is a promising upcoming biomarker that could help us guide treatment but needs proper clinical trial designs, e.g., escalation and de-escalation strategies
- One size may not fit all: there is a need for inter-disciplinary clinics with expertise
Presented by: Monika Joshi, MD, MRCP, Associate Professor, Division of Hematology and Oncology, Department of Medicine, Penn State Cancer Institute, Hershey, PA
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2024 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, San Francisco, CA, January 25th – January 27th, 2024
References:
- Tian Z, Meng L, Wang X, et al. Predictive Nomogram and Risk Factors for Lymph Node Metastasis in Bladder Cancer. Front Oncol. 2021;11:690324.
- Advanced Bladder Cancer (ABC) Meta-analysis Collaborators Group. Adjuvant Chemotherapy for Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis of Individual Participant Data from Randomised Controlled Trials. Eur Urol. 2022;81(1):50-61.
- Necchi A, Raggi D, Gallina A, et al. Updated Results of PURE-01 with Preliminary Activity of Neoadjuvant Pembrolizumab in Patients with Muscle-invasive Bladder Carcinoma with Variant Histologies. Eur Urol. 2020;77(4):439-46.
- Powles T, Kockx M, Rodriguez-Vida A, et al. Clinical efficacy and biomarker analysis of neoadjuvant atezolizumab in operable urothelial carcinoma in the ABACUS trial. Nat Med. 2019;25(11):1706-14.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384(22):2102-14.
- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): A multicentre, open-label, randomized, phase 3 trial. Lancet Oncol. 2021;22(4):525-37.
- Joshi M, Tuanquin L, Zhu J, et al. Concurrent durvalumab and radiation therapy (DUART) followed by adjuvant durvalumab in patients with localized urothelial cancer of bladder: results from phase II study, BTCRC-GU15-023. J Immunother Cancer. 2023;11(2):e006551.
- Powles T, Park SH, Caserta C, et al. Avelumab First-Line Maintenance for Advanced Urothelial Carcinoma: Results From the JAVELIN Bladder 100 Trial After >/=2 Years of Follow-Up. J Clin Oncol. 2023;41: 3486-3492.
- Galsky MD, Mortazavi A, Milowsky MI, et al. Randomized Double-Blind Phase II Study of Maintenance Pembrolizumab Versus Placebo After First-Line Chemotherapy in Patients With Metastatic Urothelial Cancer. J Clin Oncol. 2020;38(16):1797-806.
- van der Heijden MS, Sonpavde G, Powles G, et al. Nivolumab plus Gemcitabine-Cisplatin in Advanced Urothelial Carcinoma. N Engl J Med. 2023;389(19):1778-89.
- Christensen E, Birkenkamp-Demtroder K, Sethi H, et al. Early Detection of Metastatic Relapse and Monitoring of Therapeutic Efficacy by Ultra-Deep Sequencing of Plasma Cell-Free DNA in Patients With Urothelial Bladder Carcinoma. J Clin Oncol. 2019;37(18):1547-57.