(UroToday.com) The 2023 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 16th and 18th was host to a Keynote Session delivered by Dr. Norman Sharpless, former director of the National Cancer Institute from 2017 to 2022.
Dr. Sharpless began his presentation by giving the audience a snapshot into his career as a “public servant” and highlighted important snapshots from his experiences including working alongside Dr. Anthony Fauci to warn the public regarding the pending COVID-19 pandemic in 2019, his work on tobacco control with former president Donald J. Trump, and work with the Food and Drug Administration (FDA) to counteract the import of counterfeit medications.

“Let’s end cancer as we know it. Its within our power to do it.”- President Joseph R. Biden on February 2nd, 2022. This quote was the inspiration for Dr. Sharpless’ presentation title, and he attempted to tackle this topic in the remainder of his presentation.
Cancer research, and appropriate funding, will serve as one of the pillars to improve cancer outcomes. As demonstrated in the slide below, NCI funding has increased from $4,950 in the 2015 fiscal year (FY) to 6,913 in FY 2022. In 2016, the Obama administration launched the Cancer Moonshot to accelerate progress against cancer. The United States Congress signed into law the 21st Century Cures Act that same year, authorizing US$1.8 billion in funding for the Cancer Moonshot over seven years starting in 2017. While $1.8 billion USD seems like a significant boost, Dr. Sharpless argued that in the grand scheme of things, this amount is not enough. As seen in the orange portion of the graph below, the per year increased funding afforded by this Cancer Moonshot remains a very small proportion of the total NCI appropriations. While such efforts are welcome, and sorely needed, when compared to the overall budget needed to support NCI-funded trials, this additional financial boost unfortunately remains insufficient.
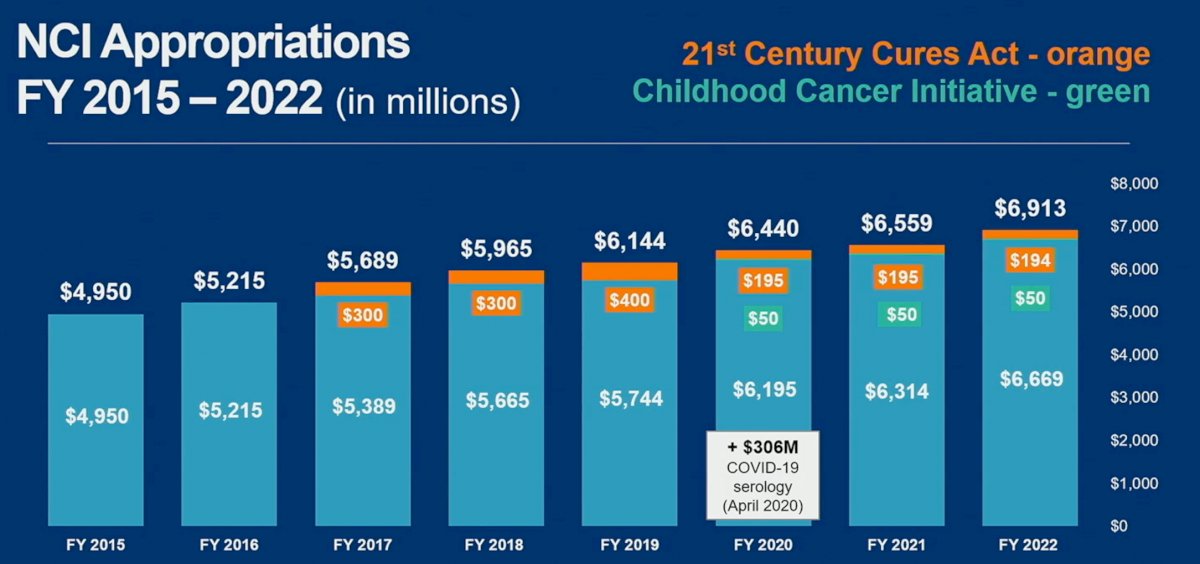
President Biden's FY23 omnibus appropriations bill will provide $1.5 billion for The Advanced Research Projects Agency for Health (ARPA-H) through FY 2025 ($500 million or a 50% increase over FY 2022), which will serve as an additional boost for NCI funding.
Over the same time frame of the last 5 years, the FDA has approved numerous new oncology-related innovations, both drug and non-drug products. As highlighted in the table below, the number of such approvals have ranged on a per annual basis from 45 in 2019 to 74 in 2021.

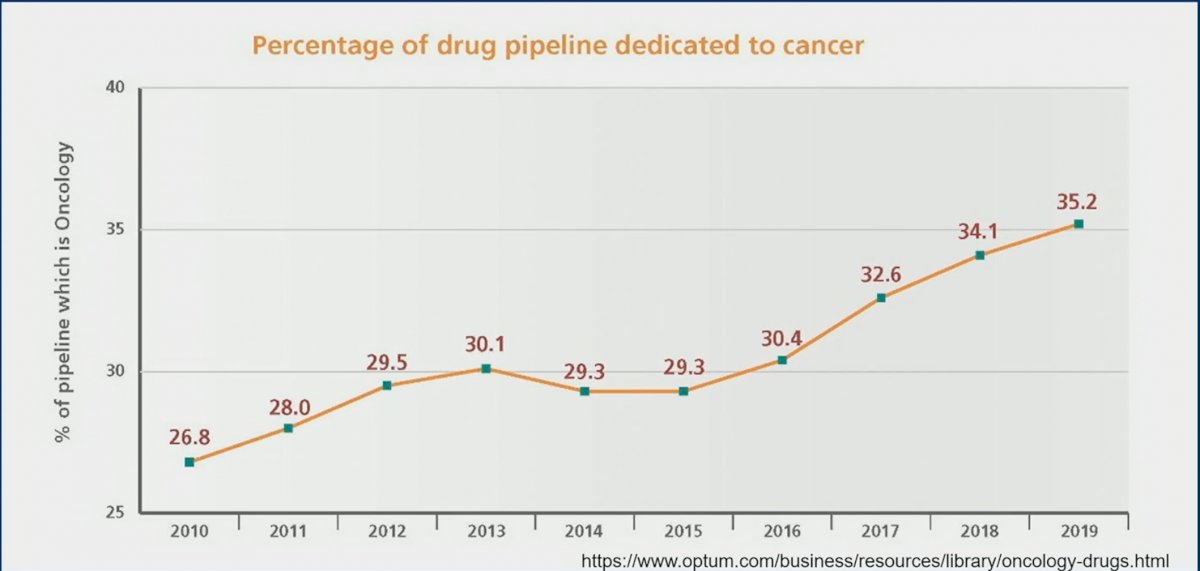
Concurrently, the percentage of drug pipeline dedicated to cancer has also seen a steady increase from 2010 (26.8%) to 2019 (35.2%).
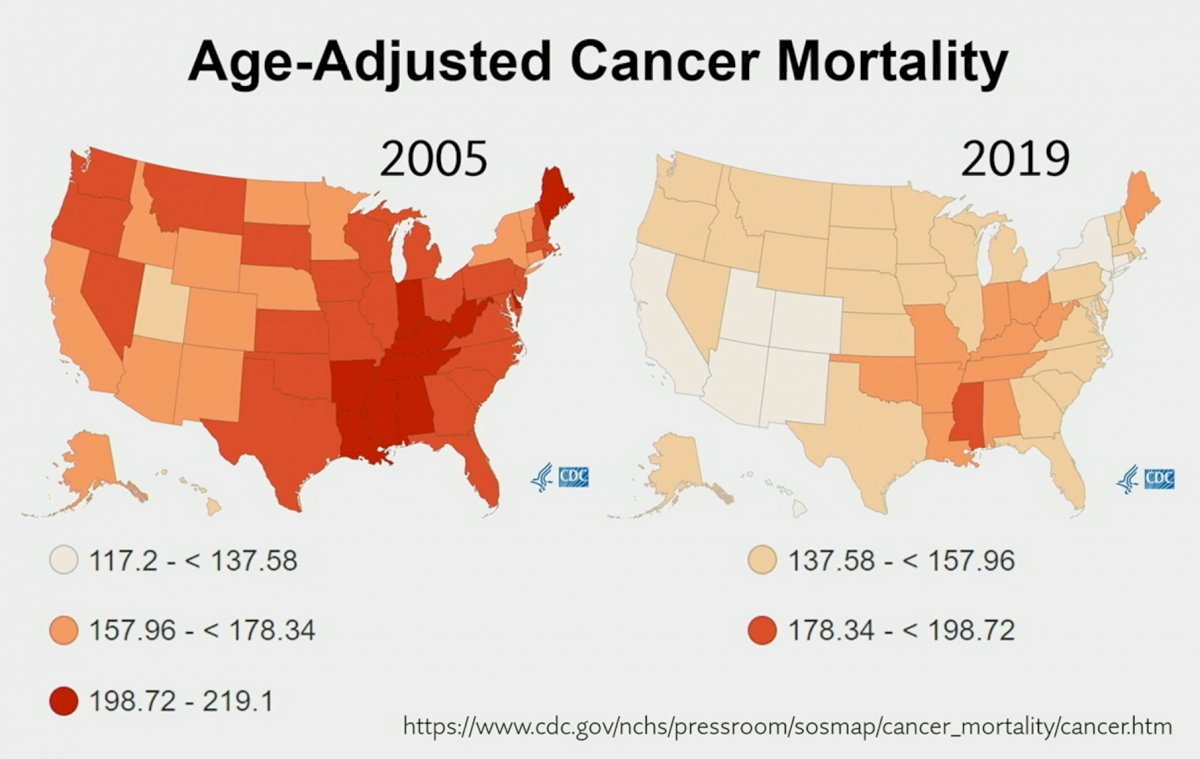
These advances, among many other reasons including improved screening and tobacco control, have seen a nationwide improvement in age-adjusted cancer mortality rates, although state-level variations remain likely due to factors such as race, socioeconomic disparities, and rurality differences.
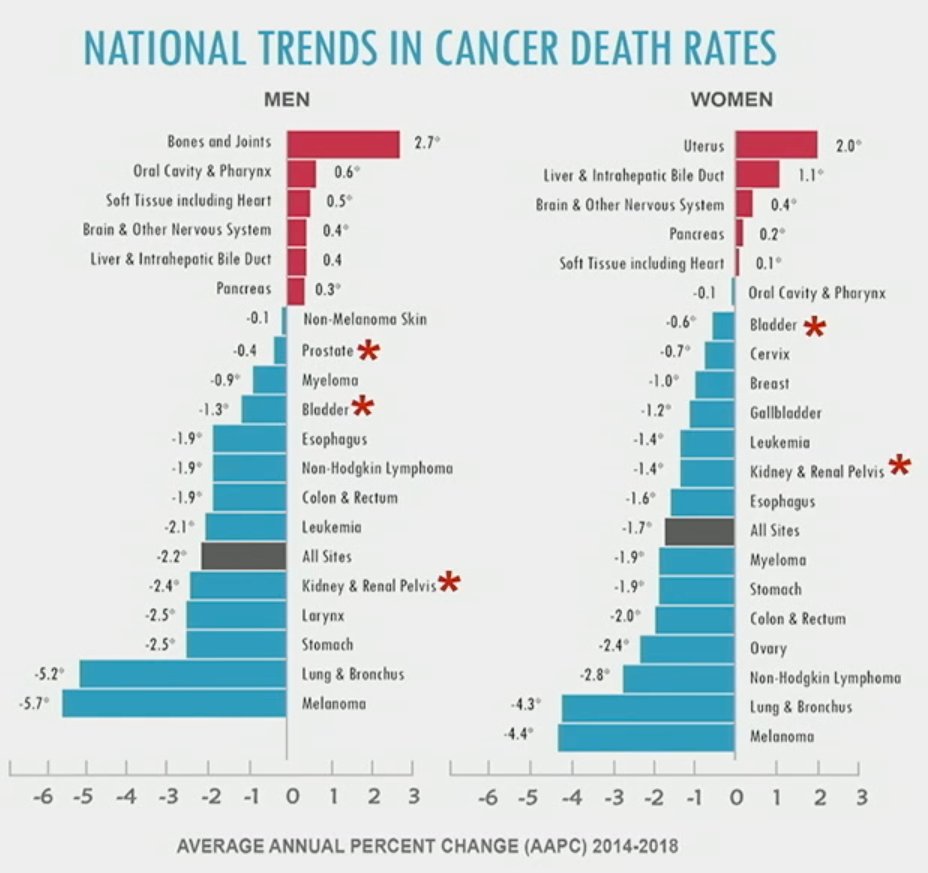
In considering President Biden’s lofty goal of dramatically reducing cancer mortality by 50% in 25 years, we need to further dissect trends in individual malignancies. As demonstrated below, we have seen impressive decreases in cancer death rates for patients with melanoma and lung/bronchial cancer in the order of a 5-6% annual percent decrease, the figures are less promising for patients with malignancies of the uterus, pancreas, and liver. All three of these malignancies are strongly related to obesity. As such, efforts to control the obesity epidemic are critical to improving cancer outcomes for such disease sites, and Dr. Sharpless believes that stronger efforts to address this issue are sorely needed.
On a positive note, Dr. Sharpless highlighted that racial disparities, with regard to cancer mortality, appear to be narrowing with African American patients seeing a more dramatic decrease in nation-level age adjusted moralities since 2000.

While Cancer Stats 2023,1 demonstrate an improvement in cancer site-related mortalities, Dr. Sharpless emphasized that these declines in overall mortality are valid only through 2020 (takes two to three years to accurately compile the data). He also pointed out the following concerns of his:
- The aftermath effect of the pandemic is yet to be fully appreciated
- The trend of obesity-associated cancers (e.g. uterine) remain concerning
- Prostate cancer mortality trends improved from 1990 to the mid 2010s; however, since then we see a concerning flattening of the curve, potentially related to decreased screening efforts based on the puzzling USPSTF recommendations during that decade

While we have seen a 33% cancer-related mortality decline, what are the remaining problems:
- Low paylines
- Ongoing threats to the National Research Budget
- Persistent disparities (especially among rural settings)
- Regulatory backsliding
- Financial toxicity and lack of access
- Spiraling research costs
In an effort to address these concerns, the MoonShot 1.0, proposed in 2016 and started in 2017, provided a $1.8 billion effort to support cancer research. This funding is set to ‘sunset” in this 2023 FY. As such, a “super-charged” cancer moonshot, in collaboration with the NIH, DOE, CDC, FDA, CMS, HRSA, VA,, USDA, EPA, DoD, was proposed by President Biden, and new NCI support should start in FY 2024.

This viewpoint has been shared by members of both major political parties, with a recent opinion piece by Senator Chris Coons from Delaware (member of Democratic party) and Senator Jerry Moran from Kansas (member of the Republican party) detailing why a $1-billion boost to the NCI “will help us beat cancer”.
In 1990, there were 215 deaths per 100,000 people. This has improved to 146 deaths per 100,000 people in 2019. On February 2nd, 2022, President Biden stated, “The goal is to cut the cancer death rate in half in the next 25 years”. Putting these words into numbers, this would equate to 73 deaths per 100,000 people in 2044.

Again, Dr. Sharpless highlighted the disease site-specific changes in age-adjusted mortality between 1994 and 2019. While lung, breast, and prostate cancer have seen dramatic improvements, obesity-related malignancies such as pancreatic, liver, and uterine have not seen significant improvements.

How do we get to 73 deaths per 100,000 by 2047? As demonstrated in the figure below, this would require a 2.5% annual decrease in age-adjusted cancer mortality rates, which as of yet, we have been unable to achieve. Opportunities to potentially reach such a lofty goal would include:
- Continued progress on tobacco control
- Obesity control
- Better therapeutics
- Earlier detection
- Addressing disparities
- Dissemination of effective approaches
In Dr. Sharpless’ opinion, the following are threats to achieving this goal, and undermining the goals/efforts of organizations such as ASCO GU:
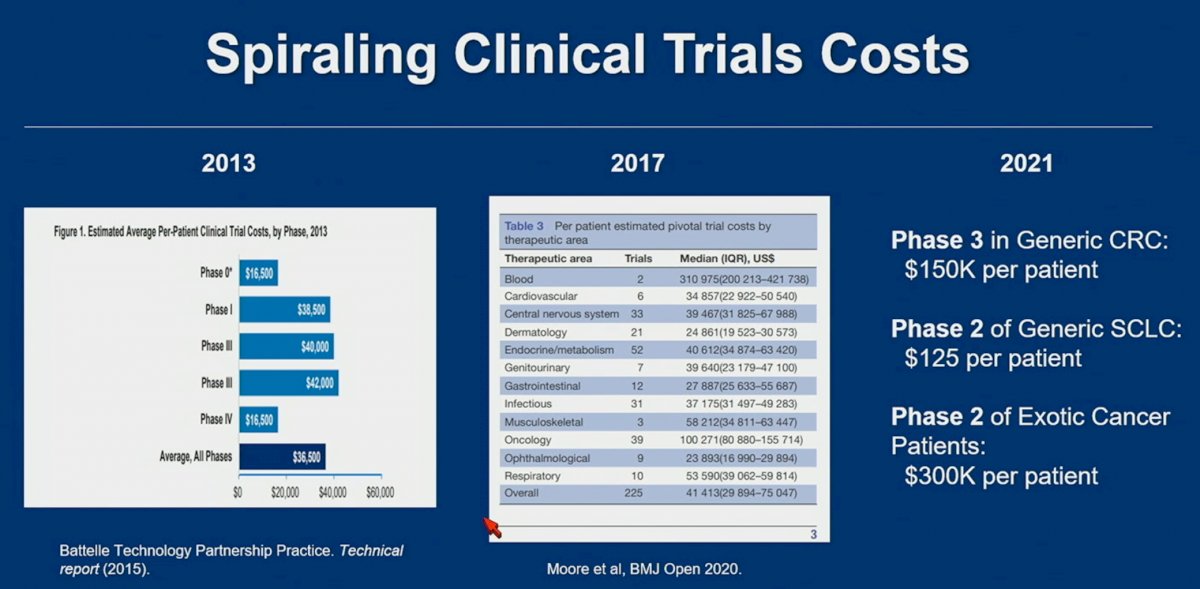
- The spiraling costs of clinical trials
- Lingering pandemic effects
- Difficulties with accelerated approval
- Issues with prior trial design and, more importantly, application of prior prostate cancer screening trials to the US population
With regards to the first point of spiraling clinical trials costs, Dr. Sharpless highlighted the significant increases in costs, even across the short time period between 2013 and 2021:
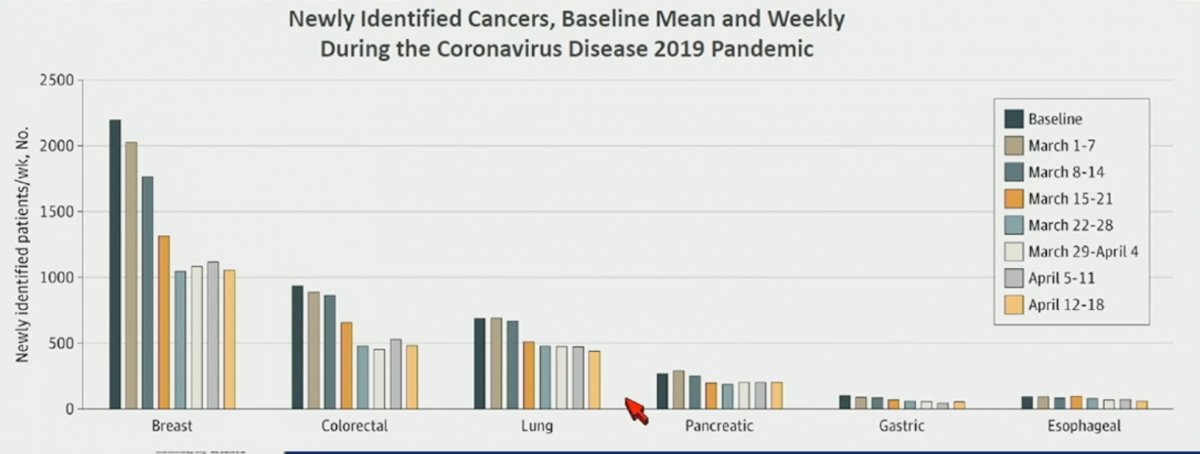
We have seen decreases in screening rates, as demonstrated for colon cancer in the graph below, which has been potentiated, in a major part, by the COVID-19 pandemic, and which is likely to lead to more advanced stages at diagnosis:

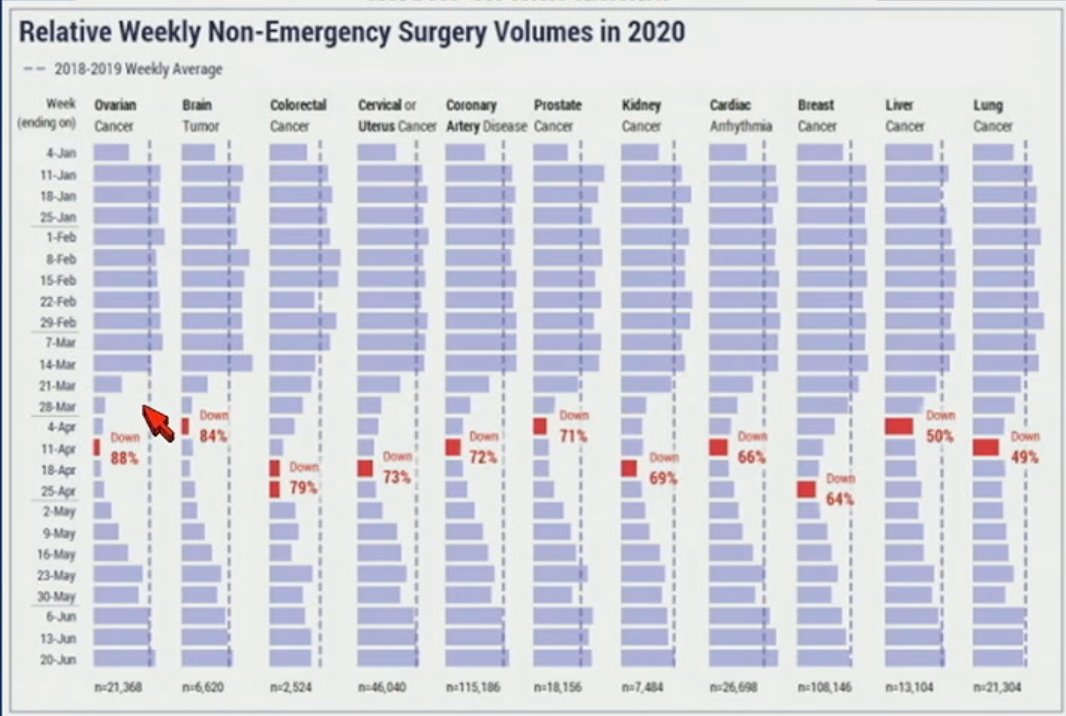
Unfortunately, this is not only limited to screening, but also to decreased surgical intervention rates:
Dr. Sharpless next touched upon accelerated approvals and noted that it was ‘under attack’. There has been interest in these accelerated approval programs since the mid 1980’s during the HIV epidemic, and clearly, the confirmatory trials for some Accelerated Approvals have taken too long. 85% of Accelerated Approval is in Cancer, which explains why there has been increased industry investment in oncology. Notable examples of GU Accelerated Approvals between 1991 and 2002 include:
- Bicalutamide 1995
- Sunitinib 2006
- Everolimus 2012
- Pembrolizumab 2020
- Rucaparib 2020
What about prostate cancer trends? US prostate cancer incidence peaked in the mid-1990’s. Concerns about overtreatment reigned in PSA screening (2008-2012), with a dramatic decline in incidence. The USPSTF has since changed recommendation to “informed decision making” in 2018. Mortality has declined sharply (3-4% annually) from 1994 to 2013 but has been essentially flat since 2013.
Dr. Sharpless concluded his Keynote speech with the following takeaways:
- There has been good progress against cancer death for three decades
- This reflects enhanced prevention, screening, treatment, and survivorship
- We still have a long way to go
- He believes that President Biden’s goal of a 50% reduction in mortality in 25 years is bold, but achievable.
Presented by: Norman E. Sharpless, MD, Former Director of The National Cancer Institute (2017 – 2022), University of North Carolina School of Medicine, Chapel Hill, NC
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, Thurs, Feb 16 – Sat, Feb 18, 2023.
References:
- Siegel RL, et al. Cancer Statistics, 2023. CA Cancer J Clin 2023;73(1):17-48.