(Urotoday.com) On the first day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2023 focussing on prostate cancer, Dr. Cameron Herberts presented in Poster Session A on a machine-learning approach to predict the utility of circulating tumor DNA for somatic genotyping in advanced prostate cancer.
Increasingly, ctDNA genotyping is being used to evaluate patient eligibility for genomics-driven treatments (e.g., PARP inhibitors) in metastatic castration-resistant prostate cancer (mCRPC). However, the clinical utility of this approach is limited by low ctDNA-fraction (ctDNA%) which may result in false negatives. Thus, the authors investigated whether a machine-learning model exploiting routine clinical prognostic markers can predict if a mCRPC patient will have sufficient ctDNA% for informative ctDNA testing.

To do so, the authors analysed plasma cell-free DNA (cfDNA) collected at baseline prior to first-line therapy from 463 consecutive patients with mCRPC. The ctDNA fraction (ctDNA%) was quantified using somatic allele frequencies and genome-wide copy number profiles via deep targeted sequencing. The authors developed a XGBoost model (70:30 train-test split) using 18 clinical factors to predict synchronously measured ctDNA% (binary classification >2% or ≤2%, i.e., the conventional ctDNA% limit of detection for mutations employed by commercial tests), with performance evaluated using area under the curve (AUC) of receiver operating characteristics.
Among enrolled men, the median age was 73 (range: 45-98) and 86% of patients had good performance status (ECOG 0-1). The median ctDNA% was 5% (range: 0-89%) and correlated with serum and radiographic metrics of disease burden, including total cfDNA concentration (ng/mL of plasma, reflecting cfDNA released by both normal and tumor cells; Spearman ρ=0.55), alkaline phosphatase (ALP) per upper limit of normal (ULN) (ρ=0.46), lactate dehydrogenase (LDH) per ULN (ρ=0.41), PSA (ρ=0.3), presence of liver metastases, and ≥10 bone lesions.
The authors trained an XGBoost model incorporating these and 13 additional clinical factors. In doing so, they achieved an AUC for ctDNA >2% of 0.83 (F1 score: 0.79). SHAP interpretability scores indicated that cfDNA concentration most strongly informed prediction of ctDNA >2%, followed by ALP/ULN and PSA, whereas features associated with initial prostate cancer diagnosis (Gleason Grade Group, de novo versus metachronous M1 disease) were less informative.
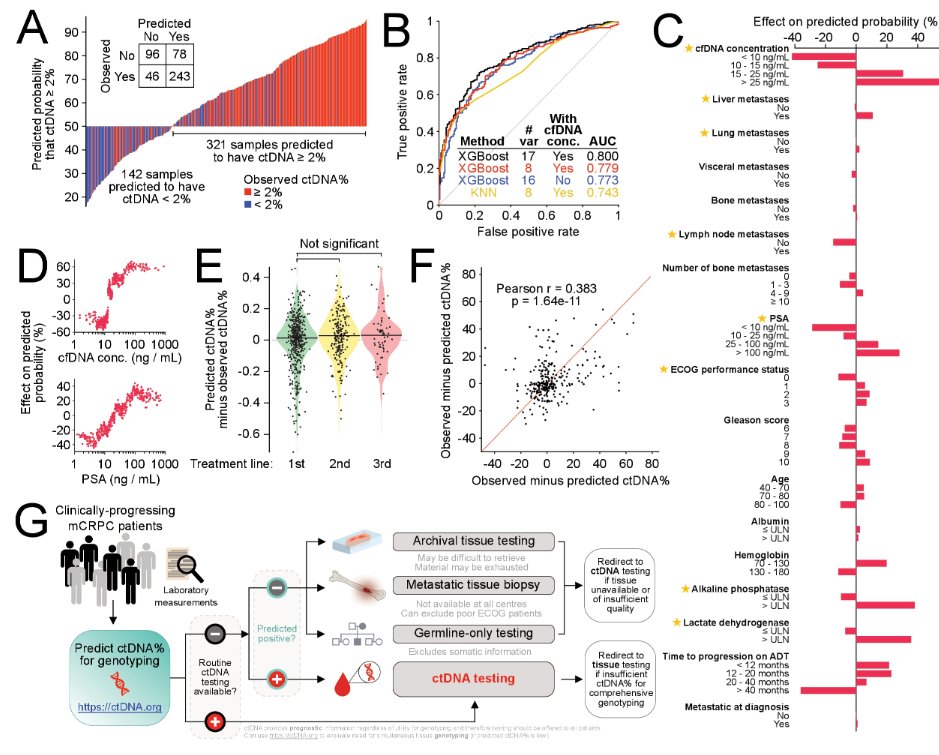
Recognizing that comprehensive and standardised clinical annotation is not always available in real-world settings, the authors further built a secondary parsimonious ctDNA%-prediction tool restricted to 8 highly informative and clinically practical factors (cfDNA concentration, ALP/ULN, LDH/ULN, PSA, albumin, ECOG, liver metastases, lung metastases) and flexible to incomplete input data, achieving a comparable AUC for ctDNA>2% of 0.76.
Additionally, the authors found that ctDNA fraction was correlated with traditionally accepted clinical markers of tumor aggressivity including de novo metastatic disease, Gleason Grade group, mCSPC treatment intensification, time from ADT initiation to development of mCRPC, metastasis location and number of bone lesions. However, even after accounting for these ctDNA fraction was independently associated with treatment outcomes.

The authors therefore concluded that this analysis supports the feasibility of a machine learning framework to estimate ctDNA% in patients with mCRPC. This point-of-care tool would enable prioritisation of mCRPC patients for ctDNA somatic genotyping with a predicted ctDNA >2%, versus tissue or germline-only testing in patients with a predicted ctDNA ≤2%.
Presented by: Cameron Herberts, BSc, PhD (c) | Vancouver Prostate Centre, Department of Urologic Sciences, University of British Columbia