(UroToday.com) The 2023 GU ASCO annual meeting included an oral abstract prostate cancer session, featuring a presentation by Dr. Daniel Spratt discussing a patient-level data meta-analysis of a multi-modal artificial intelligence prognostic biomarker in high-risk prostate cancer. Recently, a multi-modal artificial intelligence prognostic biomarker, Artera AI Prostate, was trained and validated in localized prostate cancer to more accurately risk stratify patients for multiple endpoints compared to NCCN risk groups.1 Prognostication within an NCCN risk group remains clinically important given the multiple treatment decisions required within each risk group (ie. radiotherapy dose or hormone therapy use):

At the 2023 GU ASCO meeting, Dr. Spratt and colleagues presented results validating the multi-modal artificial intelligence biomarker in high-risk prostate cancer, where an increasing number of therapeutic decisions are required.
This study used histopathology image and clinical data from patients with at least one high-risk feature (cT3-cT4, Gleason 8-10, PSA > 20 ng/mL, primary Gleason pattern 5) from six NRG/RTOG phase III randomized trials (n=1,088). Patients from two trials not part of the initial multi-modal artificial intelligence biomarker training/validation (RTOG 0521 [n=344] and 9902 [n=318]) and the multi-modal artificial intelligence validation cohort (RTOG 9202, 9408, 9413, and 9910 [n=426]) were included:
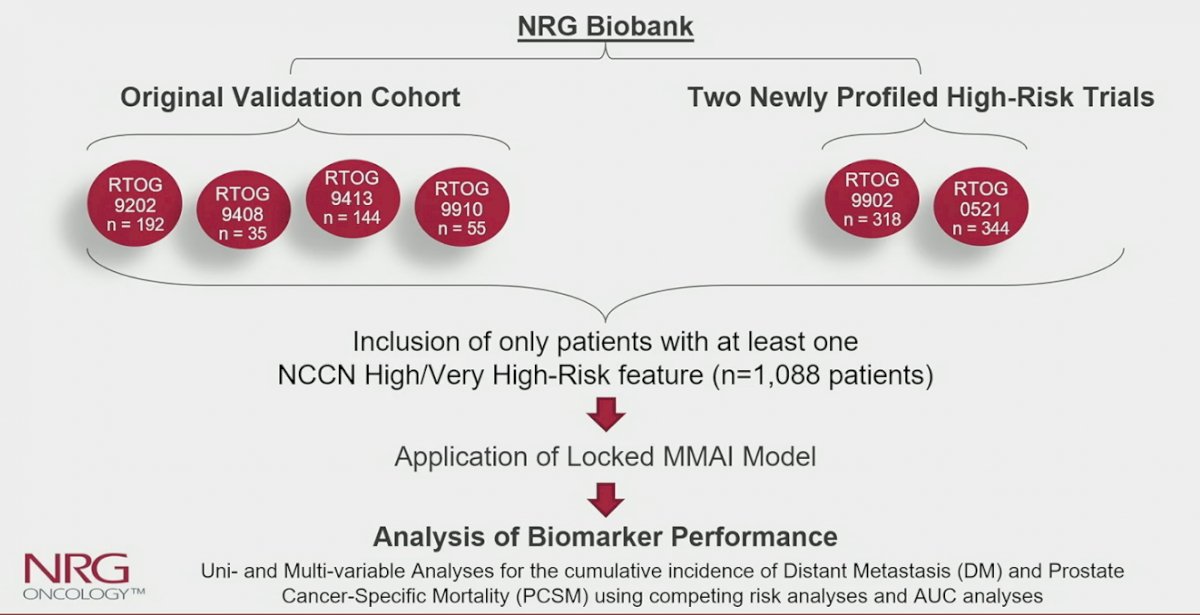
Fine-Gray, cumulative incidence, and time dependent area under the curve analyses were performed for time to distant metastasis and prostate cancer-specific mortality for standard clinicopathologic variables (age, PSA, Gleason score, T-stage, number of high-risk features) and the multi-modal artificial intelligence model, as a continuous score (per standard deviation increase) and categorically by quartile. Death from other causes were treated as competing risks.
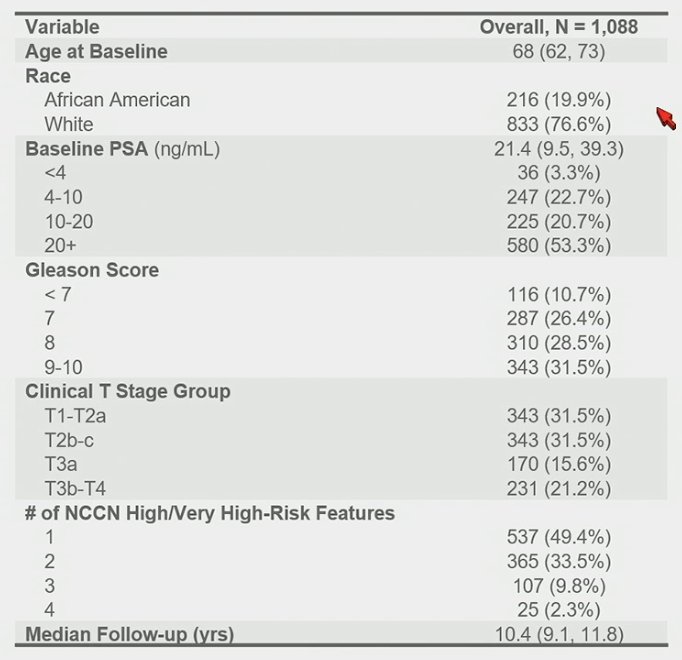
The analyzed cohort had a median follow-up of 10.4 years. The median PSA was 21 ng/mL, 60% had Gleason 8-10 disease, 37% had cT3-T4 disease, and 20% were African American. Full participant characteristics are as follows:
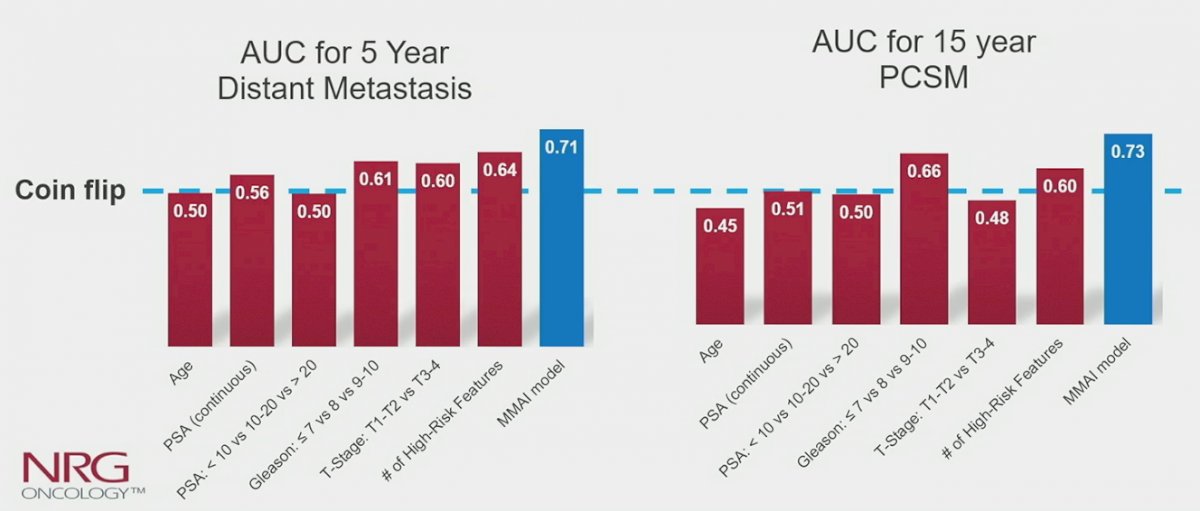
On univariable analysis, the multi-modal artificial intelligence model was significantly associated with distant metastasis (subdistribution hazard ratio [sHR] 2.05, 95% CI 1.74-2.43) and prostate cancer-specific mortality (sHR 2.04, 95% CI 1.73-2.42). On multivariable analysis, the multi-modal artificial intelligence model, adjusting for either age, PSA, Gleason score, T-stage, or number of high-risk features, was the only variable significantly associated with distant metastasis. Time dependent area under the curve was highest for the multi-modal artificial intelligence biomarker for both 5-year distant metastasis (0.71), compared to PSA (0.56), Gleason score (0.61), T-stage (0.63), or number of high-risk features (0.64), and for 15-year prostate cancer-specific mortality (0.73):
The estimated 10-year distant metastasis and 15-year prostate cancer-specific mortality rates for multi-modal artificial intelligence quartile 1 vs 4 were 8% vs 31% and 8% vs 34%, respectively:

Dr. Spratt concluded his presentation discussing a patient-level data meta-analysis of a multi-modal artificial intelligence prognostic biomarker in high-risk prostate cancer with the following take-home messages:
- This novel multi-modal artificial intelligence prognostic biomarker was successfully validated across six phase III randomized trials with long-term follow-up to be independently prognostic over standard clinical and pathologic variables for men with high-risk prostate cancer
- Despite all patients having high-risk disease, the multi-modal artificial intelligence biomarker identified those with highly variable risks for distant metastasis and prostate cancer-specific mortality
- This tool can help enable personalized, shared decision making for patients and providers
Presented by: Daniel E. Spratt, MD, University Hospitals Cleveland Medical Center, Case Western Reserve University
Co-Authors: Vinnie YT Liu, Rikiya Yamashita, Emmalyn Chen, Sandy DeVries, Ashley Ross, Angela Jia, Todd Matthew Morgan, Seth A. Rosenthal, Howard M. Sandler, Osama Mohamad, Andre Esteva, Jedidiah Mercer Monson, Steven J. Chmura, John H Carson, Alan C Hartford, Albert J Chang, Stephanie L. Pugh, Phuoc T. Tran, Felix Y Feng
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, Thurs, Feb 16 – Sat, Feb 18, 2023.
References:
- Esteva A, Feng J, van der Wal D, et al. Prostate cancer therapy personalization via multi-modal deep learning on randomized phase III clinical trials. NPJ Digit Med. 2022 Jun 8;5(1):71.