(UroToday.com) Dr. Petrilla and colleagues described time-to-event following BCG initiation for Medicare beneficiaries with intermediate to high risk NNMIBC, utilizing Centers for Medicare and Medicaid-sourced Medicare Fee-for-Service medical/pharmacy claims.
For patients with intermediate- to high-risk non-muscle invasive bladder cancer (NMIBC), the current standard of care remains transurethral resection (TURBT) followed by induction and maintenance intravesical immunotherapy with Bacillus Calmette-Guerin (BCG). We all know well the issues with the BCG shortage. And while this therapy has been around a long time, the authors claim that there is limited real world evidence or data described BCG treatment patterns and adherence to full BCG guidelines-based schedules, particularly in an older patient population.
This study describes characteristics and clinical outcomes of Medicare beneficiaries newly diagnosed with NMIBC who initiated BCG therapy following TURBT. By using this claims dataset, they are limited to patients older than 65, but potentially have greater capture of the treatment related events.
Their study was a retrospective cohort study using Centers for Medicare and Medicaid-sourced Medicare Fee-for-Service medical/pharmacy claims (100% sample). Patient selection criteria: ≥1 bladder cancer diagnosis 2010-2019, no prior radiotherapy, systemic therapy, cystectomy, or metastasis in 6 months post-diagnosis, continuously enrolled in Medicare ≥12 months pre- and post-index (or death). Index date = date of first BCG instillation. A literature-based definition for adequate maintenance BCG defined adequate (≥7 instillations of BCG within 274 days of BCG initiation) and inadequate (remainder) BCG therapy for patient stratification.
They defined the following events: time to BCG discontinuation, radical cystectomy, systemic therapy, radiation, and metastasis.
They note up front that provider access to BCG (due to supply shortage), patient tolerability, and NMIBC risk status are not captured in claims data.
Full consort diagram is noted below:
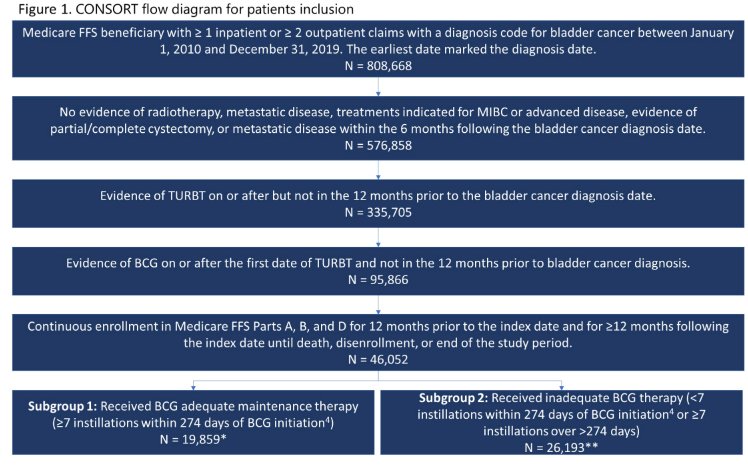
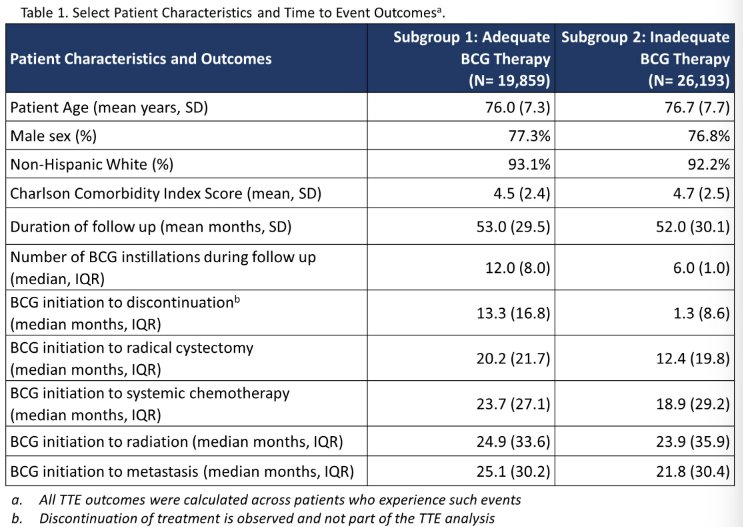
Of the 46,052 BCG-treated patients eligible for analysis, 19,859 (43.1%) received adequate BCG therapy. The two cohorts had similar baseline characteristics (Table below) and median duration of follow up (46 months). Median (interquartile range [IQR]) time from NMIBC diagnosis to BCG initiation was 2.8 (8.2) months for adequate, 3.7 (14.4) months for inadequate BCG. Time from BCG initiation to discontinuation, radical cystectomy, systemic therapy, radiation, and metastasis are reported in the table.
The authors conclude that:
- 57% of Medicare patients initiating BCG following diagnosis of NMIBC and TURBT may not have received adequate BCG therapy
- Patients with inadequate BCG therapy had numerically shorter time to radical cystectomy, systemic therapy, radiation, and metastasis than those with adequate BCG therapy.
Presented by: Allison A. Petrilla, MPH | Inovalon, Inc
Written by: Thenappan (Thenu) Chandrasekar, MD – Urologic Oncologist, Associate Professor of Urology, University of California, Davis @tchandra_uromd on Twitter during the 2023 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, Thurs, Feb 16 – Sat, Feb 18, 2023.