(UroToday.com) On the first day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2022, Poster Session A focused on the care of patients with prostate cancer. Dr. Pathmanandavel presented a poster highlighting a quantitative workflow for serial PSMA PET/CT to optimize predictive and prognostic imaging biomarker capability. This work builds off of recent clinical trial data demonstrating that 177Lutetium PSMA-617 (LuPSMA) is an effective therapy for metastatic castrate-resistant prostate cancer (mCRPC). However, treatment resistance may occur and it would be helpful to better understand patterns of response and progression.
To do so, the authors utilized 56 men who were enrolled on the LuPIN study. To be eligible, men had mCRPC previously treated with taxane chemotherapy and androgen signaling inhibitor. They then received up to 6 doses of LuPSMA and a radiation sensitizer idronoxil (NOX66). Among these 56 men, 37 had 68Ga-PSMA-11 PET/CT performed at study entry and exit. For these men, individual lesions were tracked across time using Traffic Light (TL) quantification workflow to track changes in both tumor volume and intensity at a total body and lesional level. Lesions were classified as responding in green (>30% decline in volume), stable in yellow (<30% change in volume/intensity), progressive in red (>30% increase in volume/intensity, or new). The total tumor volume (TTV) was then classified into response categories based on individual lesion response: responding (green/yellow), low volume red (<50% progressive disease) or high volume red (>50% progressive disease).

These TL workflow results were then correlated with PFS and OS.
Overall, during treatment, the median PSA decline was 77% (IQR 34-92%), and 70% of men (26/37) achieved PSA response >50%. However, PSA progression occurred in 54% (20/37) at exit imaging. Median PFS was 8.6 months (95% CI 5.6-11.6) and median OS 22 months (95% CI 18.6-25.6).
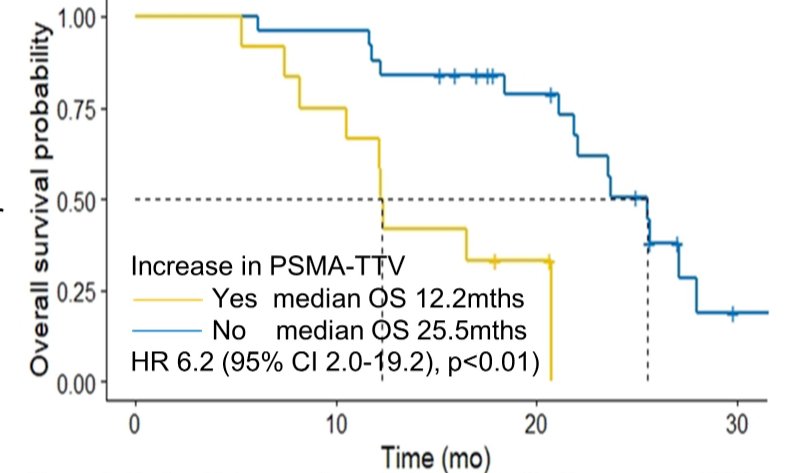
Notable, 95% of men (35/37) had reduction in PSMA SUVmax (-26.1 (IQR +11.7 to -89.4)) and SUVmean (-3.3 (+2.9 to -14.2)). However, changes in SUVmax or SUVmean were not associated with PFS or OS. In contrast, PSMA total tumor volume reduced in 68% (25/37) (median -0.64 liters (range +1.44 to -1.1)). An increase in total tumor volume was associated with worse overall survival (HR 6.2, 95% CI 2.0-19.2).
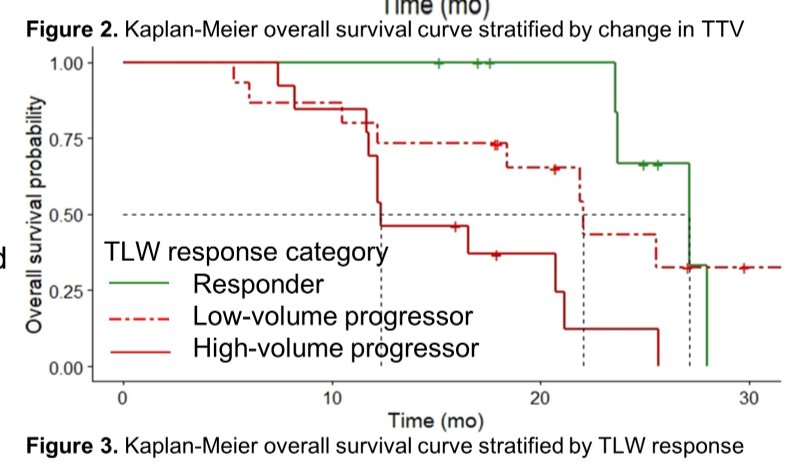
Correspondingly, on TL workflow, 24% of men (9/37) had responding/stable disease (green/yellow), 76% (28/37) had progressive disease (red) of whom 41% (15/37) had low volume progression and 35% (13/37) high volume progression. Men with high volume progression had worse OS compared to responders (HR 0.18 (0.05-0.59), p 0.005), and low volume progression (HR 0.30 (0.11-0.80), p 0.02).
Interestingly, while 68% (19/28) had progression on both TL workflow and PSA, 32% (9/28) had progression on TL workflow without PSA progression. In multivariable analysis, TL workflow and PSA progression at time of exit scans were independent predictors of OS.
Thus, the authors conclude that this study demonstrates the feasibility of characterizing lesional response on molecular imaging with a quantification TL workflow for patients being treated with LuPSMA. TL workflow response independently correlated with survival outcomes, indicating serial PSMA PET has prognostic biomarker potential.Presented by: Sarennya Pathmanandavel MPH, MBBS, Department of Theranostics and Nuclear Medicine, St Vincent's Hospital, Sydney, Australia