(UroToday.com) On the first day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2022, Poster Session A focused on the care of patients with prostate cancer. Dr. Sayegh presented a poster focusing on outcomes among patients with metastatic castration-sensitive prostate cancer (mCSPC) who do not achieve an undetectable PSA response following treatment with intensified therapy. It is known that patients who achieve a PSA nadir ≤0.2 ng/mL “anytime” after the start of treatment following intensified ADT for mCSPC have a significantly better prognosis than those who do not. The authors sought to validate these findings in a real-world population.
To do so, the authors performed a retrospective cohort study of men with mCSPC undergoing intensified ADT with either docetaxel or novel hormonal therapy (NHT) started within 3 months of diagnosis. Further patients had to have relevant data available regarding PSA nadir and tumor comprehensive genomic profiling (CGP) prior to the start of ADT. Variants of unknown significance and genomic aberrations present in <5% of patients were excluded. The authors defined their exposure as an optimal PSA response of PSA≤0.2 ng/mL. They then examined the association between optimal PSA response and progression-free survival (PFS), PCWG-2 defined PSA progression or radiographic progression or clinical progression whichever occurred first. They also assessed overall survival, defined as the time from the start of therapy to date of death or censored after last follow-up. The relationship between PSA nadir and both PFS and OS was assessed in the context of Cox proportional hazards. Gene prevalence was compared using a chi square test.
The authors identified 134 eligible patients, of whom 104 were defined as optimal responders and 30 were not. At baseline, optimal responders were somewhat younger (63 vs 65 years), had lower PSA level at the time of ADT initiation (18.1 vs 74.5 ng/mL), and were less likely to have high volume disease (48% vs 77%).
Both progression-free survival (median 60.6 vs 13.2 months, P<0.001) and overall survival (median 94.9 vs 35.2 months, P<0.001) were longer among optimal responders.
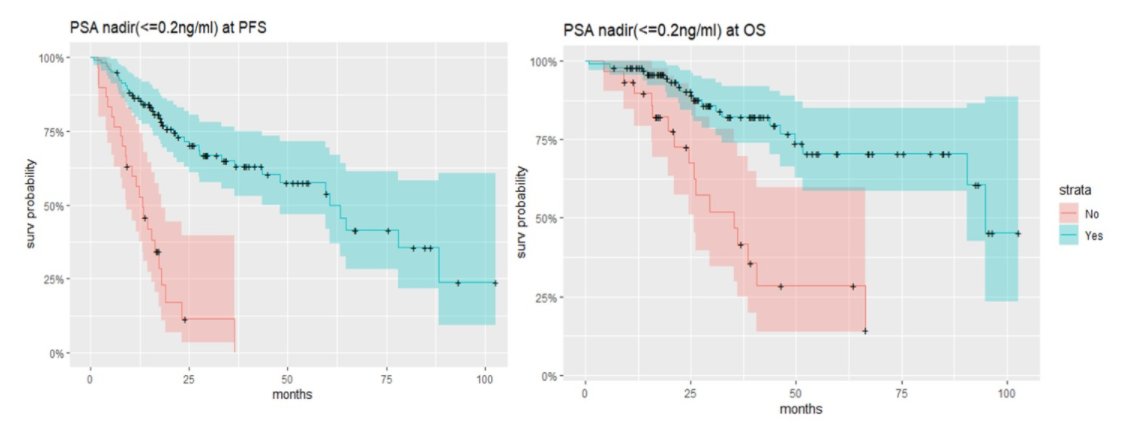
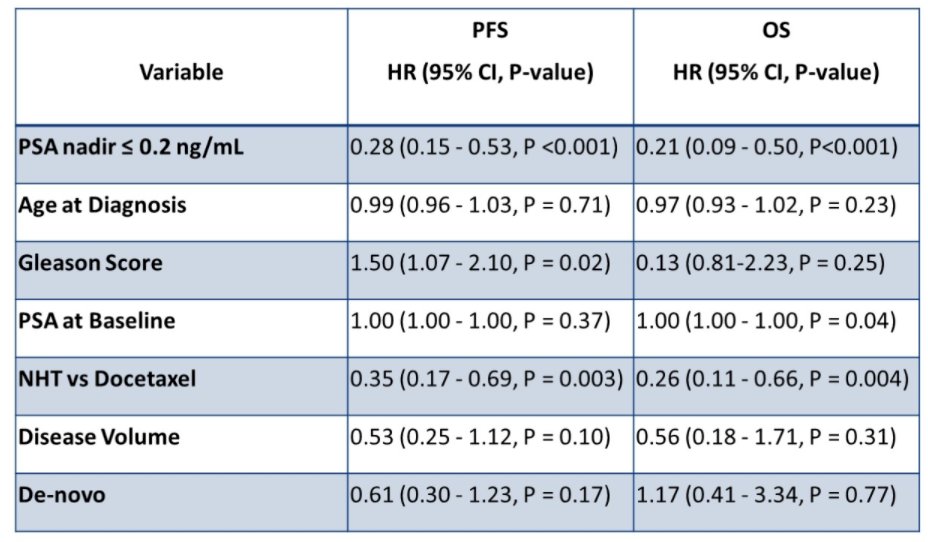
PSA response retained important prognostic information for both progression-free survival and overall survival in multivariable models.
However, the author were unable to identify any genomic biomarkers to distinguish optimal responders from those who do not achieve an undetectable nadir PSA.
They therefore conclude that, while only a minority of patients with mCSPC do not achieve an optimal PSA response with intensified ADT, these individuals have a worse prognosis.
Presented by: Nicolas Sayegh MD, Huntsman Cancer Institute-University of Utah Health Care, Salt Lake City, UT