(UroToday.com) On the second day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2022, the Rapid Abstract Session highlighted key abstract in urothelial carcinoma, including work by Dr. Galsky and colleagues who presented results of the DS8201-A-U105 trial of trastuzumab deruxtecan (T-DXd) with nivolumab in patients with HER2-expressing urothelial carcinoma (UC). Dating back almost two decades, HER2 overexpression was found in invasive UC, suggesting a role for HER2 in disease progression and prognosis. T-DXd is an antibody-drug conjugate (ADC) comprising an anti-HER2 antibody, a cleavable linker, and a topoisomerase I inhibitor payload. In preclinical models, T-DXd combined with an anti-PD-1 antibody had greater efficacy versus either agent alone. Thus, the authors performed a phase 1b, 2-part, open-label, multicenter study of T-DXd in combination with nivo in pts with HER2-expressing advanced/metastatic UC (NCT03523572).
The authors enrolled adult patients with pathologically documented advanced/metastatic UC who had centrally confirmed HER2 expression by immunohistochemistry (IHC) 2+/3+ (cohort 3; high expression) or IHC 1+ (cohort 4; low expression) who had received prior platinum-based therapy with documented progression.
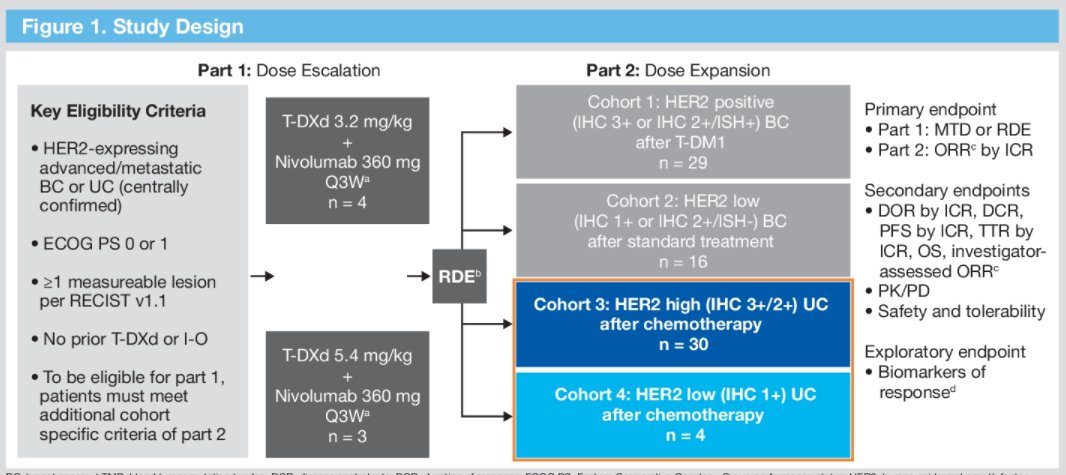
Patients were treated with T-DXd at 5.4 mg/kg and nivolumab 360 mg IV every 3 weeks (recommended dose for expansion) and were assessed for the primary endpoint of confirmed objective response rate (ORR) assessed by independent central review (ICR) per Response Evaluation Criteria in Solid Tumors version 1.1. Additional secondary endpoints (assessed by ICR) included duration of response (DOR), progression-free survival (PFS), time to response (TTR), and overall survival (OS), and safety.
With a primary analysis data cut-off of July 22, 2021, 34 patients (cohort 3, n = 30; cohort 4, n = 4) received T-DXd and nivolumab. The median age of included patients was 70.9 years (range, 41.4-80.5) and the vast majority (88.2%) were male. Further, 61.8% had received ≥1 prior regimens for locally advanced/metastatic disease and 26.5% had a history of liver metastases.
The median treatment duration in all patients was 3.2 months (range, 1-21) for T-DXd and 4.1 months (range, 1-20) for nivolumab.
In cohort 3, the objective response rate by ICR was 36.7% (95% CI, 19.9-56.1) with four patients experiencing complete response (13.3%) and 7 experiencing partial response (23.3%). The median DOR was 13.1 months (95% CI, 4.1- NE) and progression-free survival was 1.9 months (95% CI 2.7-14.4).

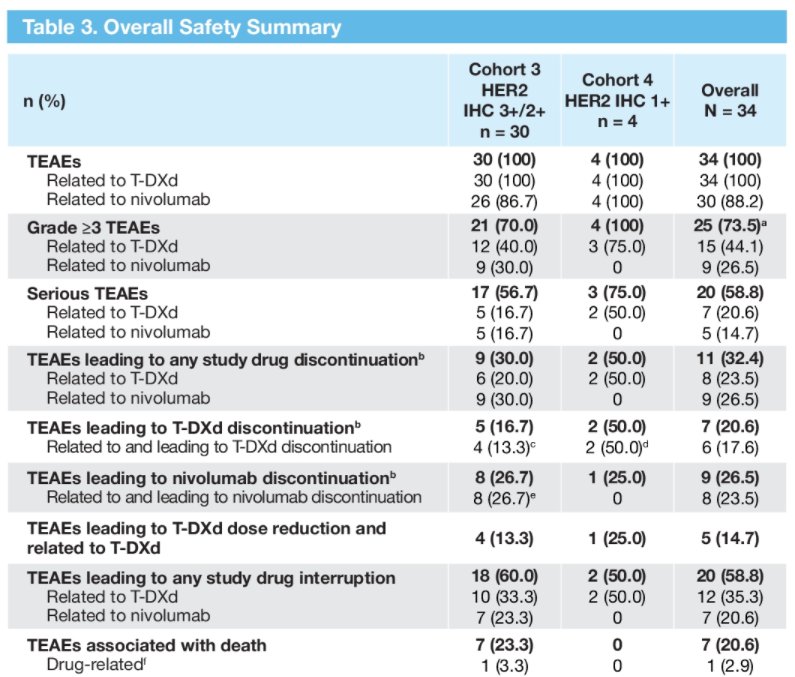
Notably, treatment-emergent adverse events (TEAEs) were seen in all patients, with grade ≥3 events in 73.5% of all patients (44.1% related to T-DXd; 26.5% related to nivolumab). TEAEs leading to drug discontinuation occurred in 32.4% of all patients (17.6% related to T-DXd; 23.5% related to nivolumab). The most common any-grade TEAEs were nausea (73.5%), fatigue (52.9%), and vomiting (44.1%). Adjudicated drug-related interstitial lung disease (ILD)/pneumonitis occurred in 23.5% of all pts (2 Grade 1 events; 4 Grade 2 events; 1 Grade 3 event; and 1 Grade 5 event).
An exploratory biomarker analysis did not show any differences in ORR based on PD-L1 expression level. However, there was numerically higher numbers of responders among those with high tumor mutational burden.
The authors concluded the combination of T-DXd with nivolumab showed antitumor activity in patients with high-expressing HER2 UC. Ongoing clinical trials are further exploring the role of T-DXd in this population.