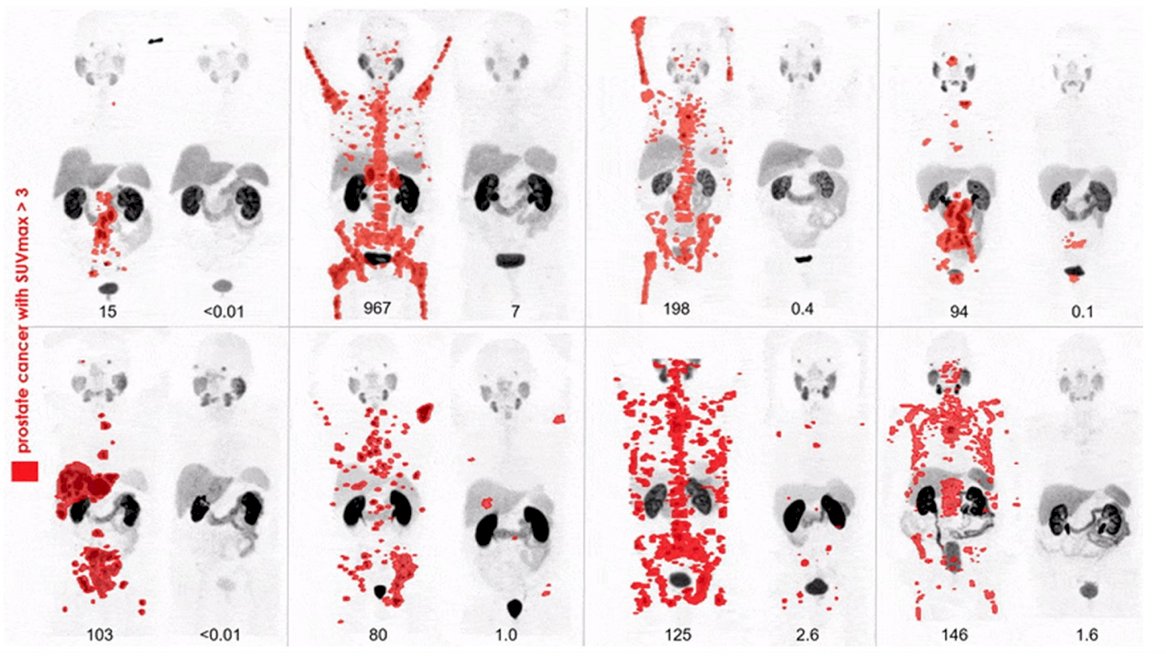
(UroToday.com) The 2022 GU ASCO Annual meeting included a session on novel treatment implementation focusing on PSMA targeting and beyond, with a presentation by Dr. Johannes Czernin discussing mechanisms of resistance to radiopharmaceuticals. Dr. Czernin started his presentation by emphasizing that we can have remarkable treatment responses to 177Lu-PSMA-617, as highlighted by the following pre- and post-177Lu-PSMA-617 treatment:
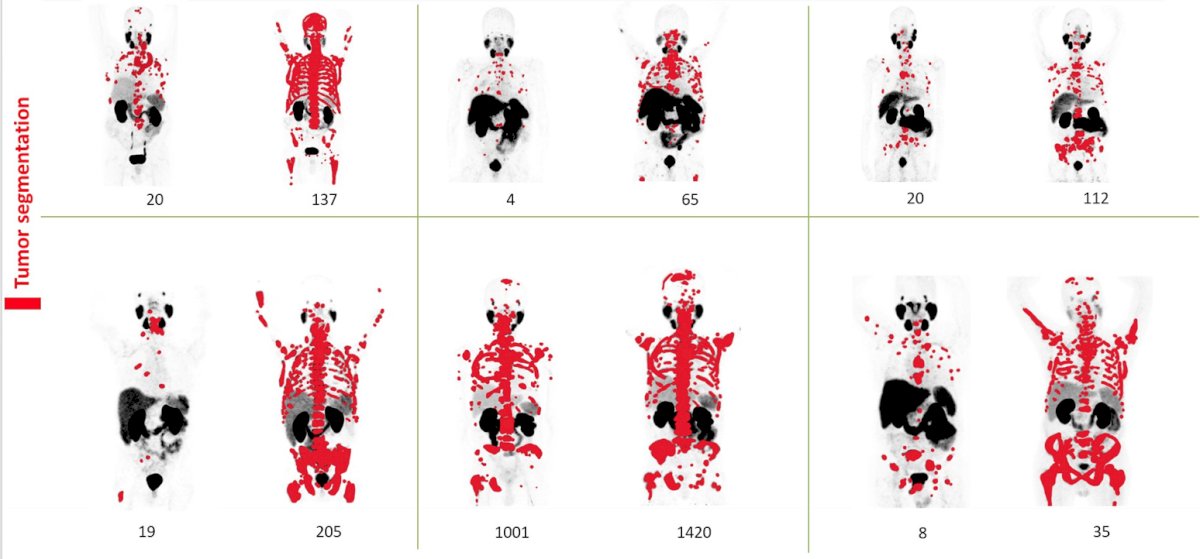
However, dramatic resistance to 177Lu-PSMA-617 is also possible as highlighted by the following pre- and post-177Lu-PSMA-617 treatment imaging:
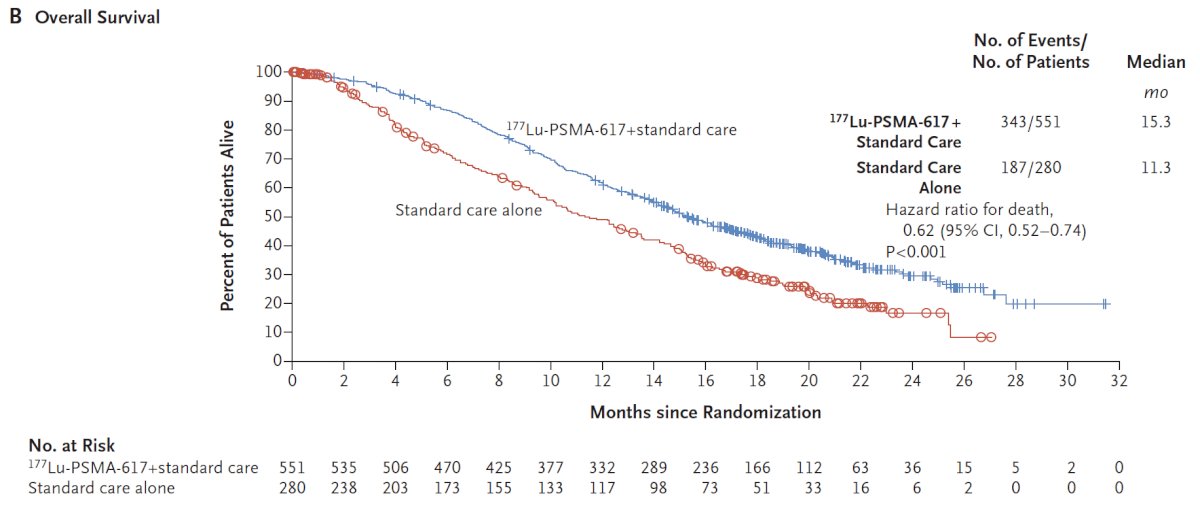
Dr. Czernin noted that the VISION trial was an international, randomized, open-label phase III study evaluating 177Lu-PSMA-617 in men with PSMA-positive metastatic castration-resistant prostate cancer who had previously received treatment with next-generation androgen receptor signaling inhibition (abiraterone, enzalutamide, etc) and one or two prior lines of taxane chemotherapy.1 Following enrollment, patients were randomized in a 2:1 fashion to receive either 177Lu-PSMA-617 (7.4 GBq every 6 weeks x 6 cycles) plus standard of care or standard of care alone. Among 1,179 screened patients, the VISION trial enrolled 831 patients, including 551 patients were allocated to 177Lu-PSMA-617 + standard of care and 280 were allocated to standard of care only. Over a median study follow-up of 20.9 month, treatment with 177Lu-PSMA-617+ standard of care significantly improved overall survival by a median of 4.0 months (median overall survival, 15.3 vs 11.3 months; HR, 0.62 [95% confidence interval 0.52, 0.74]; p < 0.001, one-sided), compared to standard of care alone, in the overall cohort of all randomized patients (n=831):
The second alternate primary endpoint showed that treatment with 177Lu-PSMA-617 + standard of care significantly improved radiographic progression free survival by a median 5.3 months (median radiographic progression free survival, 8.7 vs 3.4 months; HR, 0.40 [99.2% confidence interval: 0.29, 0.57]; p < 0.001, one-sided). However, Dr. Czernin emphasized that 50% of patients are non-responders, and all patients eventually relapse of their disease.
There is evidence from preclinical models and clinical data of several potential mechanisms of resistance and perhaps ways of overcoming resistance:
- Suboptimal patient selection – low target (PSMA) expression, heterogeneous target expression, and mutation status (ie. p53)
- Suboptimal radiation therapy – type of radiation and injected activity
- Biological tumor resistance mechanisms – (phospo)-proteomics, signaling (ie. DNA damage repair, etc), and immune-response to radioligand therapy
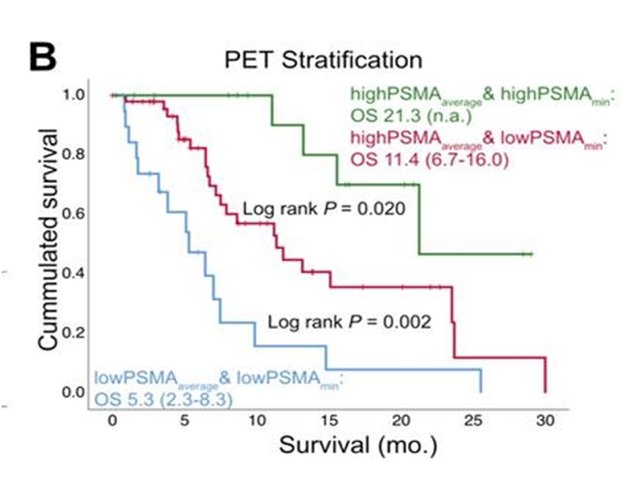
Dr. Czernin notes that targeting expression and heterogeneity matter and that clinical evidence suggests that PSMA expression/heterogeneity are correlated with 177Lu-PSMA response:
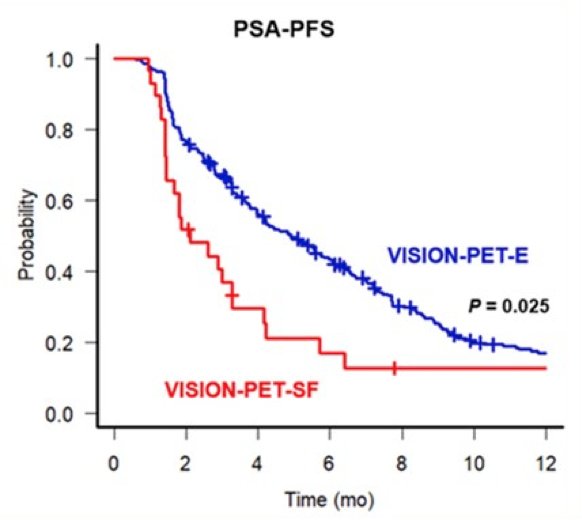
In work presented at GU ASCO 2022 and currently in press at J Nucl Med, Hotta et al. assessed the outcome of patients treated with 177Lu-PSMA who would have been screen failure by VISION-PET criteria. VISION-PET-screen failure criteria were defined as: (1) absence of metastatic lesion with uptake > liver background (i.e., low PSMA expression) or (2) presence of ≥ 1 metastatic lesion measurable by CT (≥ 1 cm for bone lesions with soft-tissue component (M1b) and solid/visceral organs lesions (M1c); ≥ 2.5 cm for lymph nodes lesions (N1-M1a)) with uptake ≤ liver background (i.e., PSMA-negative lesions). Overall, 272/301 (90.4%) of the analyzed patients were VISION-PET-eligible while 29/301 (9.6%) were VISION-PET-screen failure: 8/301 (2.7%) with low PSMA expression and 21/301 (7.0%) with PSMA-negative lesions, respectively. Over a median follow-up time of 12.6 months (IQR: 7.0-21.3, range: 0.6-62.3), VISION-PET-screen failure patients had a worse median PSA PFS (2.1 months (95% CI 1.1-3.3) vs. 4.1 (95% CI 4.0-5.8); p = 0.025)) vs VISION-PET-eligible patients:
Dr. Czernin also highlighted that mutational status matters given that p53 mutations create resistance to external beam radiotherapy, and p53 loss renders prostate cancer resistant to PSMA radioligand therapy. Furthermore, several additional mechanisms that may matter to treatment sensitivity are as follows:
- Radiation type – 177Lu-PSMA (beta-emitter) vs 225AC-PSMA (alpha emitter)
- Injected activity (“dose”) – particularly for 225AC-PSMA
- Tumor absorbed dose
- DNA damage response
Dr. Czernin concluded his presentation of mechanisms of resistance to radiopharmaceuticals by highlighting potential remedies to resistance in this landscape:
- Suboptimal patient selection:
- Low target (PSMA) expression, heterogeneous target expression the role of imaging, FDG, PSMA
- Mutation status (ie. p53) the role of genetic genotyping
- Suboptimal radiation therapy – type of radiation and injected activity the role of industry and the portfolio of isotopes (225Ac, 90Y, 212Pb), and the role of professional societies for demanding dosimetry
- Biological tumor resistance mechanisms – (phospo)-proteomics, signaling (ie. DNA damage repair, etc), and immune-response to radioligand therapy the role of basic/translational sciences
Presented by: Johannes Czernin, MD, University of California—Los Angeles, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, Thursday Feb 17 – Saturday Feb 19, 2022
References: