(UroToday.com) The 2022 GU ASCO Annual meeting included a session on novel treatment implementation focusing on PSMA targeting and beyond, with a presentation by Dr. Himisha Beltran discussing biomarker testing in the era of novel therapeutics. Dr. Beltran notes that, as we saw in the TheraP trial,1 not all patients with PSMA-positive disease identified by PET respond to PSMA-directed therapy. Furthermore, approximately 15-20% of patients with late-stage castration-resistant prostate cancer have PSMA-low or PSMA-negative disease. There are several important aspects to patient selection for PSMA-directed therapy, including: (i) expression of the target (PSMA), (ii) other biomarkers of response (tumor features, drug features, and drug mechanism), and (iii) mechanisms of disease resistance (to guide next therapy).
The first challenge of biomarker testing in the era of novel therapeutics is that PSMA can be heterogeneous in individual patients. Additionally, PSMA can also be heterogeneous within individual lesions, thus we do not know how ‘much’ PSMA is required for optimal and durable therapy response, which may also depend on the type of PSMA-targeted therapy. Heterogeneity of PSMA may also be seen across metastases in individuals, giving credence to the seed vs soil hypothesis based on work from Dr. Beltran’s lab showing that a PSMA-low metastatic lesion can generate PSMA-low metastases in vivo.
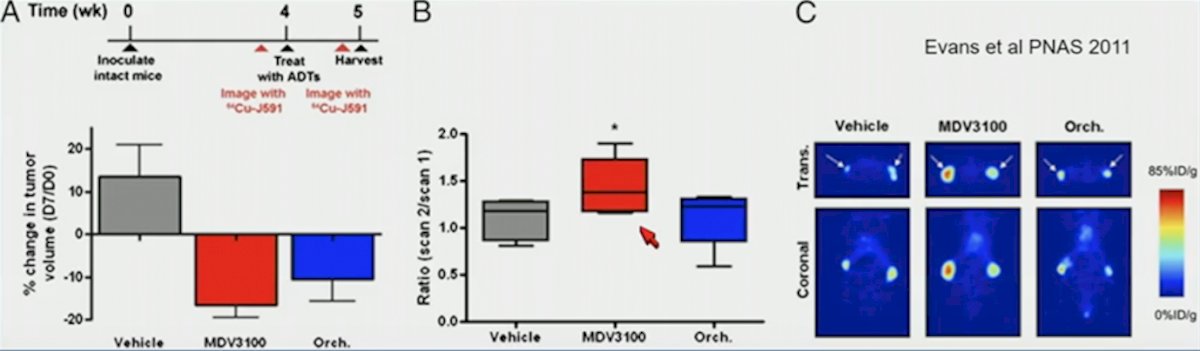
The second challenge of biomarker testing in the era of novel therapeutics is that PSMA is dynamic in individual patients. PSMA dynamics on androgen receptor therapies include: (i) increased expression with acute androgen receptor inhibition, (ii) rapidly decreased expression with treatment response, (iii) increased expression in androgen receptor-drive castration-resistant prostate cancer, and (iv) lost in a minority of patients with late-stage castration-resistant disease. Enzalutamide results in decreased tumor volume but an increase in PSMA in hormone-sensitive prostate cancer preclinical models:
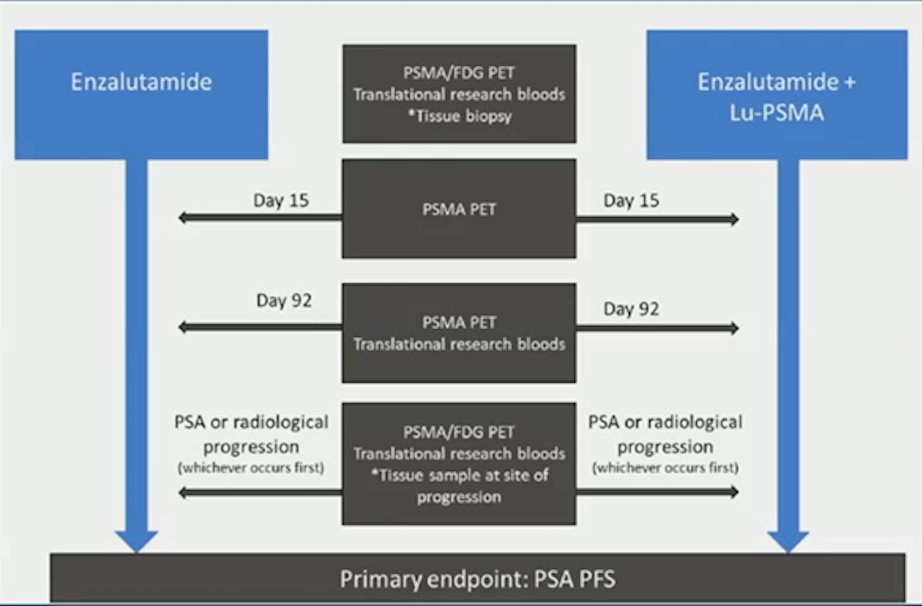
Additionally, a number of clinical studies have been conflicting in metastatic hormone-sensitive prostate cancer and metastatic castration-resistant prostate cancer, either showing an increase in PSMA or a decrease in PSMA expression after ADT/ARPI with PET/CT imaging approximately one month after therapy. As such, more data is needed to further elucidate this relationship. The ENZA-p trial assessing enzalutamide with Lu-PSMA-617 versus enzalutamide in men with metastatic castration-resistant prostate cancer includes serial imaging plus liquid biopsies, allowing for valuable prospective assessment of PSMA dynamics in the metastatic castration-resistant setting, as well as association of PSMA dynamics with tumor features. The trial design for ENZA-p is as follows:
The third challenge of biomarker testing in the era of novel therapeutics is that PSMA is lost in come patients with late stage castration-resistant prostate cancer. PSMA is expressed in >90% of metastatic hormone-sensitive prostate cancer and in 70-80% of late-stage castration-resistant prostate cancer. How and why is PSMA expression “lost”? Perhaps this is secondary to (i) loss of differentiation, (ii) loss of the androgen receptor (an indirect regulator of PSMA), (iii) epigenetic reasons, or (iv) other unknown mechanisms. Indeed, work from Dr. Beltran’s group has shown that PSMA can be lost in androgen receptor-negative small cell neuroendocrine prostate cancer. Additionally, PSMA negative castration-resistant prostate cancer may be FDG positive, with PSMA/FDG discordant disease historically associated with a poor prognosis.
Dr. Beltran then asked the question “Should we select ‘out’ patients with AR-negative castration-resistant prostate cancer or neuroendocrine prostate cancer for consideration of PSMA therapy?” Her group is working on answering several of these open-ended questions: (1) Rather than PSMA-radioligands, what other radioligands may be applied for molecular imaging and therapy of neuroendocrine prostate cancer? (2) Is there any PSMA-positive sub-population among neuroendocrine prostate cancer to benefit from PSMA-targeted imaging and therapy? Alternative regulation of PSMA may include (similar to the androgen receptor) HOXB13 binding to a PSMA enhancer and regulating PSMA expression. In the absence of the androgen receptor, HOXB13 may still be a regulator of PSMA. As follows are several additional open-ended questions as posed by Dr. Beltran:
- Does androgen receptor amplification/androgen receptor overexpression/androgen receptor splice variants equal increased PSMA expression which may equal response or resistance to PSMA therapies?
- Does RB1 and TP53 loss of cfDNA methylation changes (associated with lineage plasticity) equal lower PSMA and thus equal resistance to PSMA therapies?
- Do PTEN/PI3K/AKT aberrations associate with higher PSMA activity (as supported by preclinical data)?
- Do DNA repair aberrations associate with response to PSMA radionuclides (synthetic lethality)?
- How does ctDNA tumor content and/or circulating tumor cells at baseline and on therapy associate with PSMA-quantified (PET) tumor burden in patients?
Currently, we lack systematic studies that address the diverse mechanisms of resistance that occur in these patients. If resistance is still PSMA positive, this could guide sequencing of PSMA drugs, including 225Actinium, antibody-drug conjugates, BiTE and other T cell engagers, CAR-T and others. If resistance is no longer PSMA positive, the mechanism of resistance is important, which may guide patient selection for alternative targets. Alternative radiopharmaceuticals to the beta-emitting 177Lu-PSMA-617 targeted radioligand therapy include the utilization of alpha particles. The rationale for the utilization of alpha particles is a higher linear energy transfer, with a shorter range of effect. Clinical reports are still limited/preliminary and mainly include 225Act-PSMA-617, which has shown potential activity in patients resistant to 177Lu-PSMA-617 targeted radioligand therapy2 and in patients with CNS disease.
Dr. Beltran concluded her presentation with the following take-home messages:
- The optimal response to PSMA-directed therapy likely depends on:
- Expression of the target (PSMA) – which can be heterogeneous within and across metastases, dynamic during androgen receptor blockade, and during castration-resistant prostate cancer and neuroendocrine prostate cancer evolution. The biology is complex and not all androgen receptor-negative disease will be PSMA-negative
- Biomarkers of response – may be influenced by both tumor factors (androgen receptor status, plasticity, DNA repair) and drug mechanism (radiation, immune)
- Mechanisms of resistance – PSMA-positive resistance may be targetable with novel PSMA-directed approaches, but it is unclear how often PSMA-negative disease occurs
- Other cell surface targets may complement PSMA to improve patient selection and inform the development of novel theranostics
- Incorporation of serial imaging and liquid biopsies into our clinical studies will be essential for improving our understanding of PSMA dynamics across diverse sets of patients to guide the development of more robust predictive biomarkers
Presented By: Himisha Beltran, MD, Dana-Farber Cancer Institute, Boston, MA
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, Thursday, Feb 17 – Saturday, Feb 19, 2022
References:
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Feuerecker B, Tauber R, Knorr K, et al. Activity and adverse events of Actinium-225-PSMA-617 in advanced metastatic castration-resistant prostate cancer after failure of Lutetium-177-PSMA. Eur Urol 2021 Mar;79(3):343-350.