(UroToday.com) In session on the third day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2022, Poster Session C focused on Renal Cell Cancer; Adrenal, Penile, Urethral, and Testicular Cancers. In this session, Dr. Albers described the results of the PRIMETEST trial of primary retroperitoneal lymph node dissection (RPLND) in stage II A/B seminoma.
This treatment approach, utilized without adjuvant local or systemic treatment, is being investigated with the goal of avoiding long-term radio- or chemotherapy–related toxicity associated with other management approaches.
The interim results of PRIMETEST (NCT 2015053664) were presented at ASCO-GU 2019. To summarize, this is a phase II single-arm, single center study of primary unilateral template RPLND (open or robotic) for patients with stage II A/B seminoma. Adjuvant therapy was not used.

Eligible patients had unilateral retroperitoneal lymph node metastases < 5 cm (stage IIA and IIB) with human chorionic gonadotropin (HCG) < 5 mU/ml and could have either been stage IIA/B at initial diagnosis, at time of recurrence under active surveillance, or after adjuvant carboplatin in clinical stage I. The phase II trial was designed to exclude the upper limit of a 95% confidence interval at 30% recurrent disease.
The trial accrual was completed in a single center between May 2016 to June 2021 with 33 consecutive patients, of whom 13 and 20 had with stage IIA and IIB disease, respectively. While 9 patients initially presented with stage II disease, 19 presented with recurrence during active surveillance and 5 had received adjuvant carboplatin prior to recurrent disease.
At time of RPLND median HCG was 0.1 mU/ml (range 0 – 2.2 mU/ml). Open and robotic RPLND was performed in 14 (42 %) and 19 (58 %) patients, respectively, with one patient converted from a robotic to open surgical approach. The median OR time was 169 min (range 101 – 351 min). Median estimated blood loss was 50 ml (range 0 – 400 ml). There were two intraoperative complications, one involving bleeding from the renal vein managed with clamping and suturing and the other a conversion from robotic to open surgery. Higher grade complications (Clavien Dindo ≥ III) occurred in 4 patients (11%; 2 x pulmonary embolism, 1 x ileus requiring small bowel resection, and 1 x lymphocele requiring draining). There were two patients readmitted I the 30 days following surgery.
The median lymph node yield was 15 (range 3 to 31) and the median number of involved lymph nodes was 1 (range 0 to 40. Notably, 9% of patients did not have evidence of disease on the RPLND specimen (CS I). Median size of metastasis on histological report was 28 mm (range 11 – 69 mm)
With a data cut-off of January 2022, the median follow-up was 30 months (range 6-56). Two patients had been lost to follow-up. Of 31 evaluable patients, 10 had recurrence disease (31%) and recurrence free survival was 69%. The median time to recurrence was 6 months (range 3 to 36 months). The recurrences included infield recurrences in 3 of 10 cases. Notably, the authors found comparable results with open and robotic surgery.
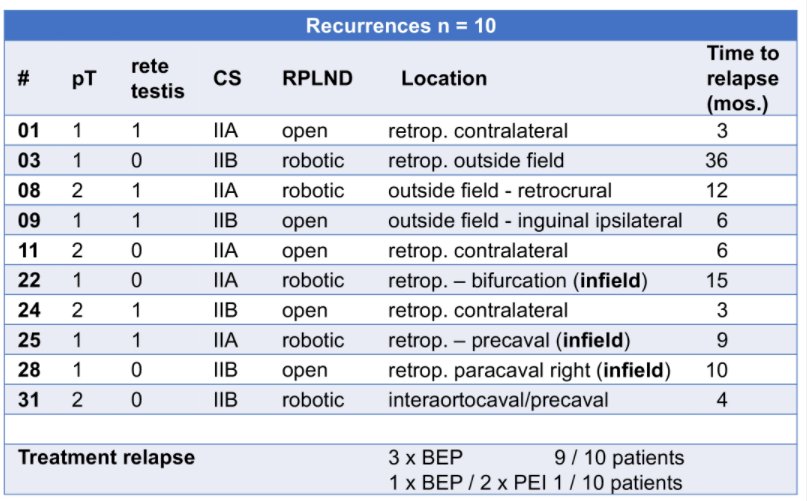
All patients with relapse underwent standard chemotherapy and are currently without evidence of disease.
Thus, the authors conclude that both open and minimally invasive surgical resection of small volume, unilateral seminoma metastasis is feasible with acceptable toxicity. Current recurrence-free survival rates suggest this approach as an option to avoid standard treatment (chemotherapy, radiotherapy) in selected patients. However, ongoing work is required to better predict who will benefit from the surgery only approach.
Presented by: Peter Albers MD, Department of Urology, Heinrich-Heine-University