(UroToday.com) The 2022 GU ASCO Annual meeting included a session on from genetic testing to systemic therapies for renal cell carcinoma (RCC), featuring a presentation from Dr. Michael Atkins and colleagues discussing the final results of HCRN GU16-260-Cohort A, a phase 2 study of nivolumab and salvage nivolumab + ipilimumab in treatment-naïve patients with advanced clear cell RCC. Nivolumab is FDA approved for patients with VEGFR TKI-resistant RCC and the nivolumab + ipilimumab combination is FDA approved for treatment naïve patients with IMDC intermediate and poor risk RCC. However, little information is available on the efficacy and toxicity of nivolumab monotherapy in treatment naïve RCC or the efficacy of nivolumab + ipilimumab salvage in patients with tumors resistant to initial nivolumab monotherapy. The initial results of HCRN GU16-260 were presented at ASCO 2020, with Dr. Atkins presenting the final clinical results at GU ASCO 2022 for Part A.
Eligible patients with treatment naïve RCC received nivolumab 240mg IV q2 weeks x 6 doses followed by 360mg IV q3 weeks x 4 doses followed by 480 mg q4 weeks until progressive disease, toxicity, or completion of 96 weeks of treatment (Part A). Patients with progressive disease prior to, or stable disease at 48 weeks were potentially eligible to receive salvage nivolumab (3mg/kg)/ipilimumab (1 mg/kg) q3 weeks x 4 doses followed by q4 week nivolumab maintenance for up to 48 weeks (Part B). All patients were required to submit tissue from a metastatic lesion obtained within 12 months prior to study entry and prior to Part B for correlative studies. The schema for the HCRN GU16-260-Cohort A trial is as follows:

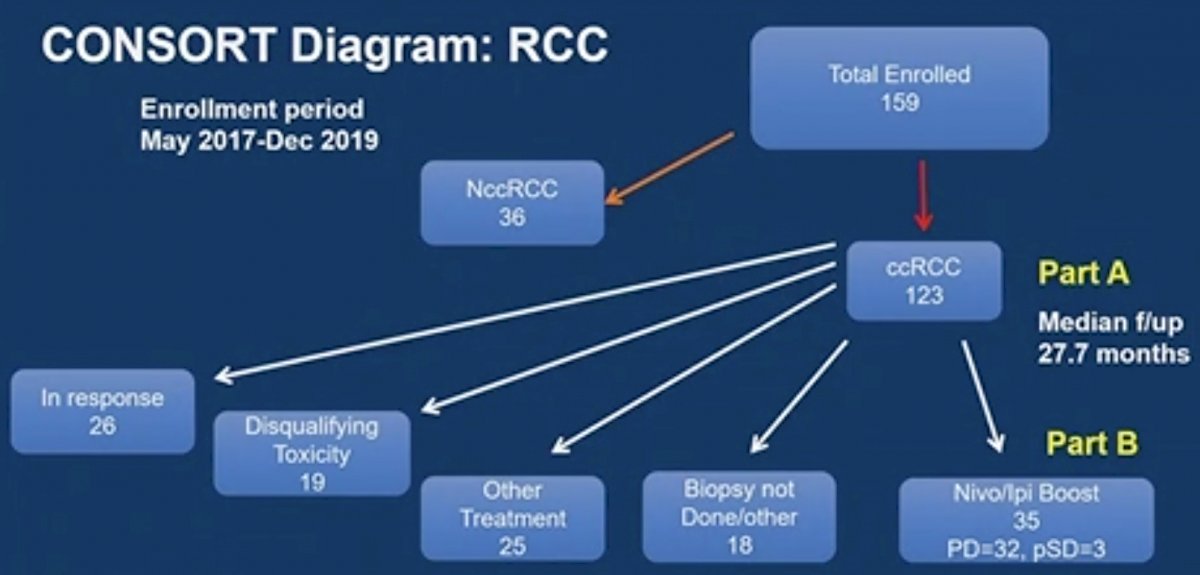
There were 123 patients with clear cell RCC enrolled between May 2017 and December 2019 at 12 participating HCRN sites. The CONSORT diagram for this study is as follows:
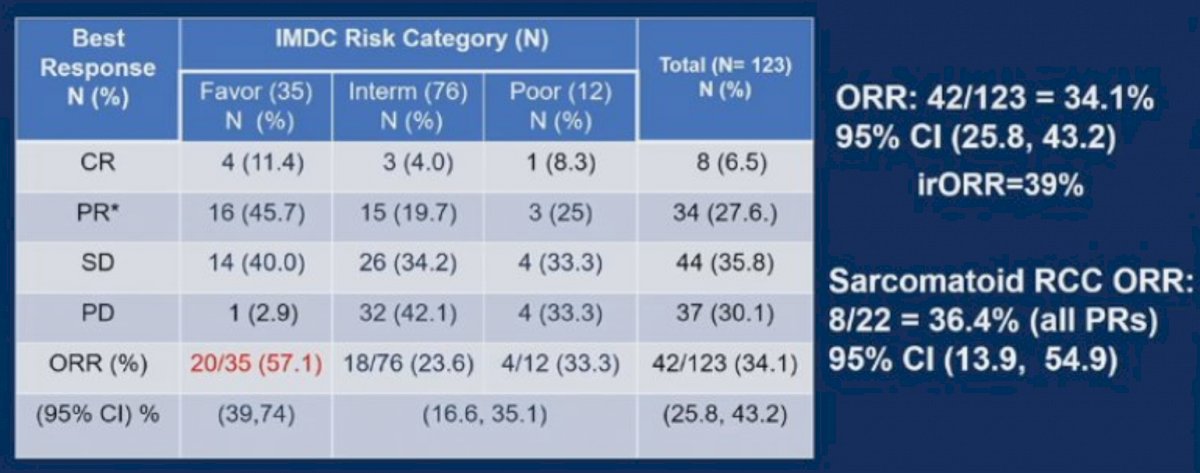
The data lock was on April 7, 2021, with a median follow-up for this trial of 26.9 months. The median age was 65 (32-86) years of age and 72% were male. There were 35 IMDC favorable risk patients (28%), 76 intermediate risk (62%), and 12 poor (10%) risk patients; 22 (18%) patients had a component of sarcomatoid histology. ORR defined by RECIST was 34.1% (95% CI 25.8-43.2%), including 6.5% with complete response, 27.6% with partial response, and 35.8% with stable disease. The ORR stratified by IMDC was 57.1% (95% CI 39-74%) for favorable risk, 25% for intermediate/poor risk, and 36.4% for sarcomatoid histology. The ORR by PD-L1 status was 21/78 (27%) for patients with tumor PD-L1 of 0, 8/16 (50%) for PD-L1 of 1-20, and 6/8 (75%) for PD-L1 of > 20% (trend test p-value 0.002). There were 5/7 (71.4%) favorable risk patients with PD-L1 > 1 that responded. A summary of the ORR’s is as follows:
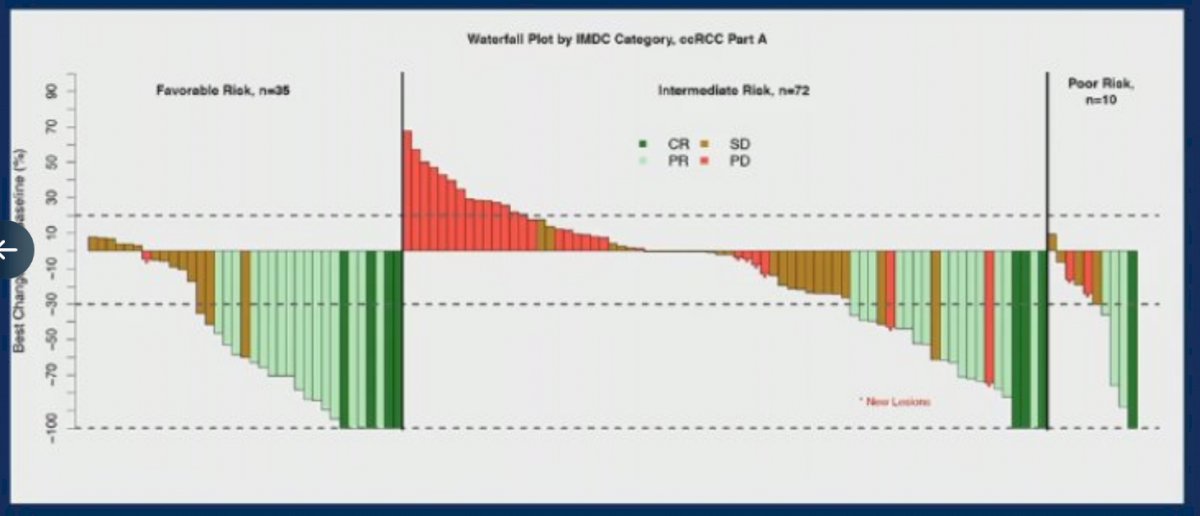
The median duration of response was 27.6 (13.7, not reached) months with 26/42 responders including 17/20 (85%) with favorable risk remaining progression free. Tumor shrinkage by IMDC risk is as follows:
The median PFS was 8.3 (5.5, 10.9) months (32.5 months for IMDC favorable risk and 5.4 months for intermediate/poor risk), and there were 91 patients that remained alive with a 24 month OS rate of 78%. There were 65 patients that were potentially eligible for salvage nivolumab + ipilimumab (Part B), but 25 did not enroll due to symptomatic progressive disease (n = 6), grade 3-4 toxicity on nivolumab (n = 17), or other (n = 2), and 5 patients were not treated due to inability to confirm residual disease on a biopsy. ORR for Part B by RECIST was 11.4% (4/35) and by irRECIST 17.2%. Grade 3-5 treatment-related adverse events (not including asymptomatic amylase/lipase) were seen in 20.3% of patients in Part A and 14.2% in Part B with one death in each cohort.
Dr. Atkins concluded his presentation of the final results of HCRN GU16-260-Cohort A with the following take home messages:
- Nivolumab monotherapy represents an alternative first-line treatment option, particularly in the ipilimumab and TKI averse patients, and among those with favorable risk disease (57% ORR, 85% ongoing responses, with rare early progressive disease)
- Nivolumab + ipilimumab is likely the preferred upfront “pure IO” regimen, particularly for IMDC intermediate/poor patients and those with sarcomatoid histology
- Salvage treatment with nivolumab + ipilimumab after nivolumab was frequently not possible and is of somewhat limited efficacy
- Tumor PD-L1 levels predicted for efficacy, however only 20% of tumors were PD-L1 positive and 60% of responses were in PD-L1 negative patients. As such, it is not useful for clinical decision making, but could be part of a multi-component biomarker
Presented by: Michael B. Atkins, MD, Georgetown Lombardi Comprehensive Cancer Center, Washington, DC
Co-Authors: Opeyemi Jegede, Naomi B. Haas, David F. McDermott, Mehmet Asim Bilen, Mark N. Stein, Jeffrey Alan Sosman, Robert S. Alter, Elizabeth R. Plimack, Moshe Chaim Ornstein, Michael E. Hurwitz, David J. Peace, Sabina Signoretti, Thomas Denize, Alessia Cimadamore, David A. Braun, Catherine J. Wu, David Johnson Einstein, Paul J. Catalano, Hans J. Hammers
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, Thursday Feb 17 – Saturday Feb 19, 2022