(UroToday.com) In an oral abstract on the third day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2022 focused on renal cell cancer, Dr. Choueiri presented 30-month follow-up from the KEYNOTE-564 trial of post-nephrectomy adjuvant pembrolizumab in patients with renal cell carcinoma (RCC).
While nephrectomy is the standard of care for patients with locoregional RCC, the risk of recurrence for patients with high-risk disease is high. Thus, adjuvant therapy has been pursued for many years. In general, adjuvant tyrosine kinase inhibitors did not offer significant clinical benefits. However, the double-blind, multicenter, randomized KEYNOTE-564 study (NCT03142334) demonstrated that adjuvant pembrolizumab in patients with renal cell carcinoma (RCC) at intermediate-high or high risk of recurrence after nephrectomy or nephrectomy and resection of metastatic lesions resulted in a statistically significant improvement in disease-free survival (DFS) vs placebo with 24 months of follow-up (HR 0.68, 95% CI 0.53−0.87; p = 0.0010).
While previously presented and published, in brief, KEYNOTE-564 enrolled patients with histologically confirmed, clear cell RCC (pT2, grade 4 or sarcomatoid, N0 M0; pT3 or pT4, any grade, N0 M0; any pT, any grade, N+ M0; or M1 NED [no evidence of disease after primary tumor and soft tissue metastases completely resected ≤1 year from nephrectomy]) who had undergone surgery ≤12 weeks prior to randomization. Patients were then randomized to receive adjuvant pembrolizumab or placebo.

The primary endpoint was DFS by investigator assessment in all randomized patients (ITT population) while overall survival in the ITT population, and safety/tolerability in all treated patients, were key secondary endpoints. While the previous publication presented results with 24 months of follow-up, this updated analysis provides an additional 60 months of follow-up to 30 months.
The KEYNOTE-564 trial randomized 994 patients in a 1:1 fashion to pembrolizumab (N = 496) or placebo (N = 498). As of data cut-off of June 14, 2021, the median (range) follow-up duration was 30.1 (20.8−47.5) months.
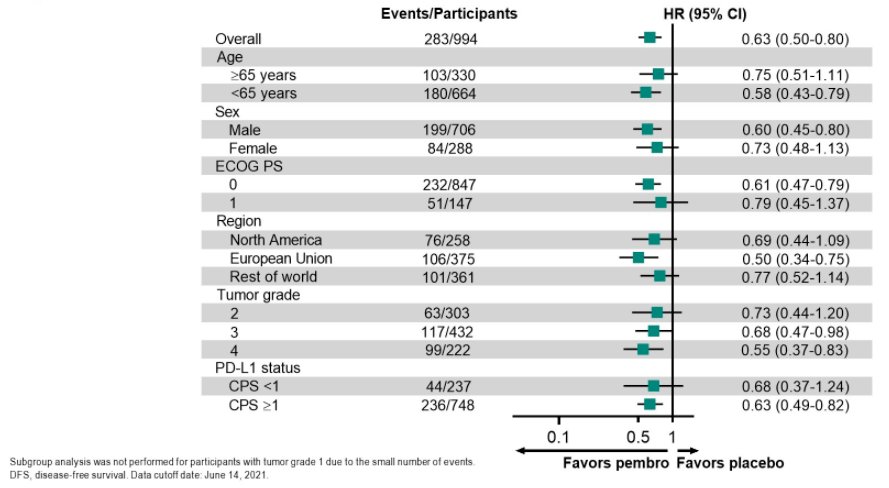
In this updated analysis, DFS benefit with pembrolizumab was maintained (HR 0.63, 95% CI 0.50−0.80; nominal P < 0.0001). The estimated DFS rate at 24 months was 78.3% with pembrolizumab vs 67.3% with placebo. Compared to the primary analysis at 24 months of follow-up, this updated analysis had very comparable findings, with a somewhat larger magnitude of effect (HR 0.63 vs 0.68).

Further, this benefit of adjuvant pembrolizumab was consistent across subgroups, including those defined by age, sex, ECOG performance status, region of residence, tumor grade, and PD-L1 status.
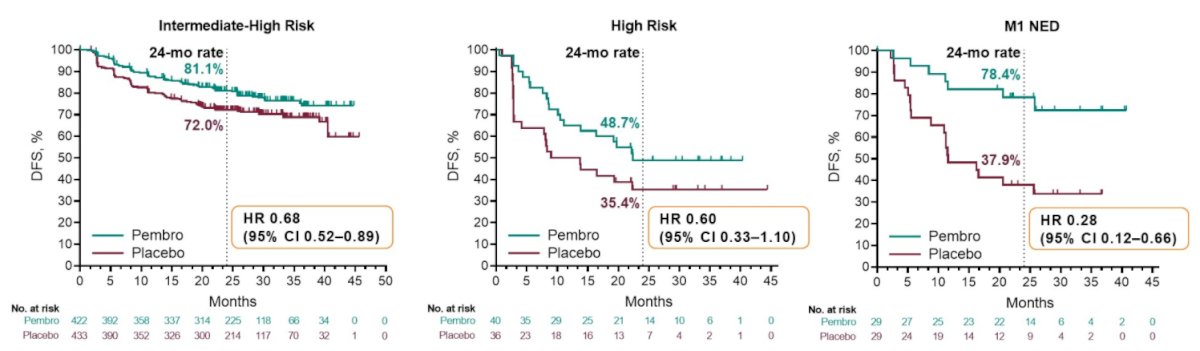
When stratified by recurrence risk subgroups, the benefit of adjuvant pembrolizumab was seen in patients with M0 disease with intermediate-high risk of recurrence (HR 0.68, 95% CI 0.52−0.89), M0 high risk of recurrence (HR 0.60, 95% CI 0.33−1.10), or M1 NED (HR 0.28, 95% CI 0.12−0.66).
The benefit of adjuvant therapy was even larger among those with sarcomatoid features (HR 0.54, 95% CI 0.29-1.00) than those without (HR 0.63, 95% CI 0.48-0.83).
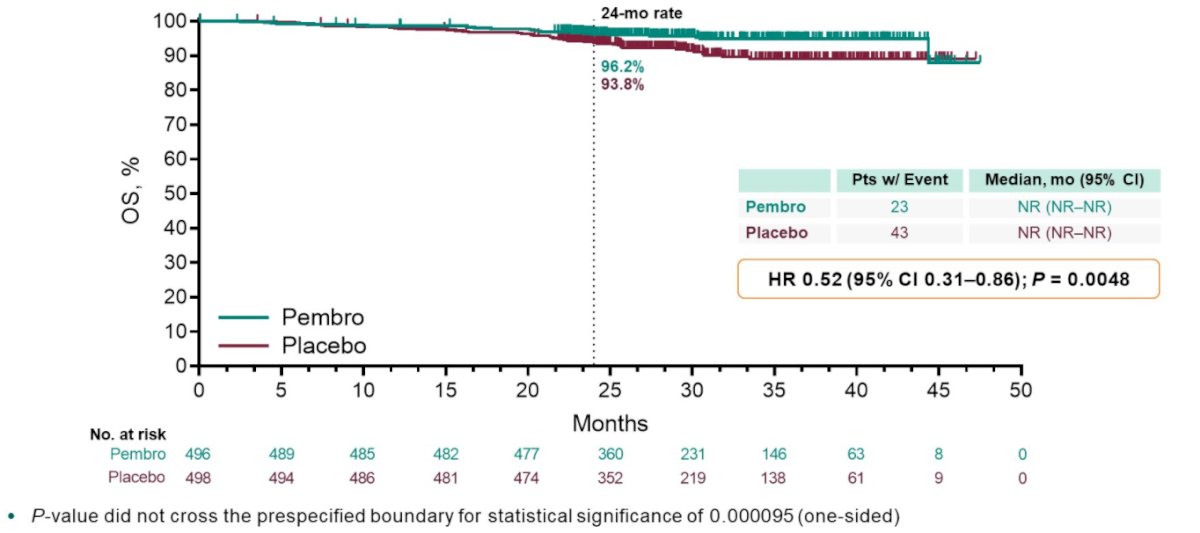
A total of 66 OS events were observed, 23 in the pembrolizumab arm and 43 in the placebo arm (HR 0.52, 95% CI 0.31−0.86; P = 0.0048), though the p-value did not cross
the statistical hypothesis testing boundary (of p=0.000095) and additional follow-up is planned for this key secondary endpoint. The estimated OS rate at 24 months was 96.2% with pembrolizumab vs 93.8% with placebo. Compared to the primary analysis, the magnitude of benefit increase somewhat with increasing follow-up.
With additional follow-up, there was no increase in any-grade or grade 3-4 adverse events or steroid use for immune-mediated adverse events observed. No deaths related to pembrolizumab occurred.

In conclusion, Dr. Choueiri highlighted that adjuvant pembrolizumab continued to demonstrate a DFS benefit following nephrectomy for intermediate-high or high risk of recurrence after surgery.
Presented by: Toni K. Choueiri, MD, Lank Center for Genitourinary Oncology, Dana-Farber Cancer Institute, Brigham and Women’s Hospital, and Harvard Medical School