(UroToday.com) In a poster presentation on the third day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2022 focussed on Renal Cell Cancer; Adrenal, Penile, Urethral, and Testicular Cancers, Dr. Aly-Khan Lalani presented the rationale and design of the CYTOSHRINK trial examining the role of cytoreductive stereotactic hypofractionated radiotherapy (SBRT) along with combination ipilimumab/nivolumab for metastatic kidney cancer.
The principle of cytoreductive in metastatic renal cell carcinoma (mRCC) was established in the interferon era with cytoreductive nephrectomy. Since that time, the SURTIME and CARMENA, conducted in the VEGF-targeted therapy era, failed to show a benefit to cytoreductive nephrectomy, thus questioning its role in contemporary management. However, the standard of care systemic therapy landscape has shifted again and, in place of tyrosine kinase inhibitors such as sunitinib, combination immune checkpoint inhibition is now the accepted first-line treatment approach. In the Checkmate-214 trial, which provided the first data for this combination immune checkpoint approach, patients with a primary kidney lesion in situ appeared to have less benefit from this approach than those who had undergone prior nephrectomy.
A less invasive alternative to cytoreductive nephrectomy is stereotactic body radiation therapy (SBRT) and may further induce an enhanced systemic anti-tumor immune response.
To assess this, the authors designed the CYTOSHRINK trial (NCT04090710). This phase II trial enrolls previously untreated patients with biopsy-proven mRCC of any histology and IMDC intermediate/poor risk disease. Patients with a primary kidney lesion 20cm or greater in size, those with a history of previous abdominal radiation precluding SBRT, or those who have a contraindication to ipilimumab or nivolumab are excluded.
Following enrollment, patients are randomized in a 2:1 fashion to ipilimumab and nivolumab plus SBRT (30-40 Gy in 5 fractions) to the primary kidney mass between cycles 1 and 2 (experimental arm, E), versus standard of care ipilimumab and nivolumab alone (standard arm, S).
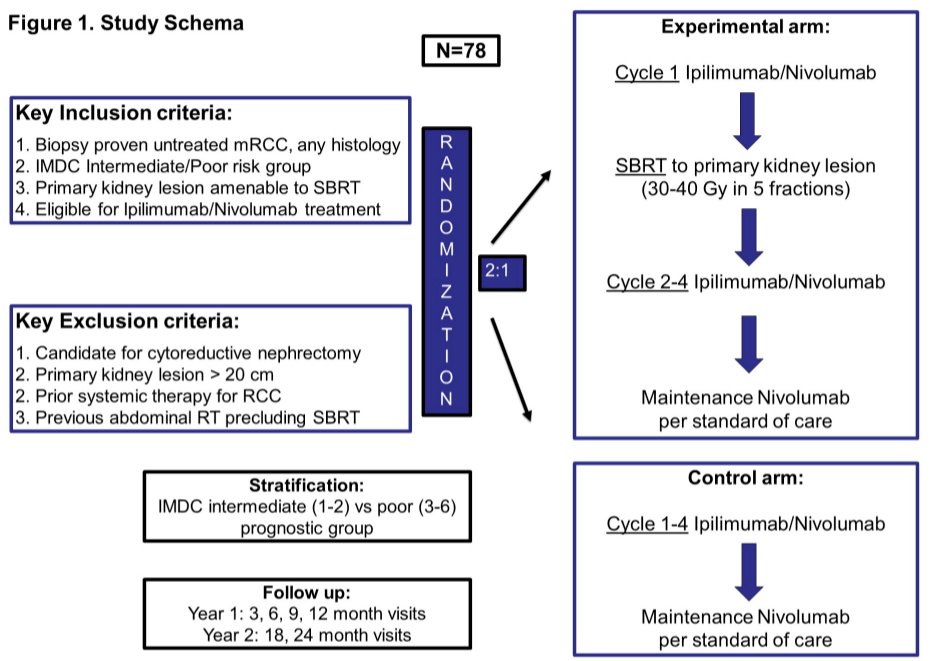
The primary objective is to compare the efficacy of ipilimumab and nivolumab plus SBRT versus ipilimumab and nivolumab alone, as determined by the hazard ratio for progression free survival (PFS). Secondary objectives include evaluation of safety and tolerability, overall survival, objective response rate, and health-related quality of life.
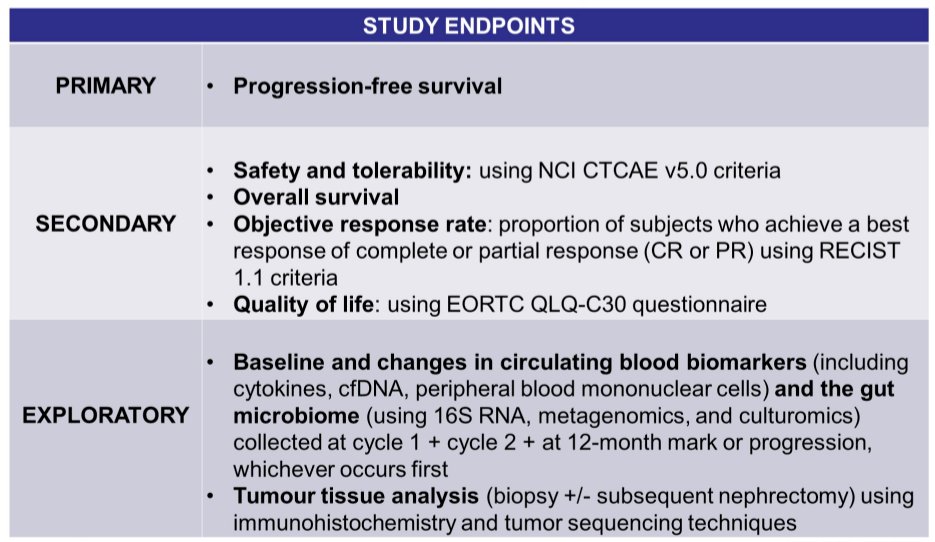
Blood and fecal samples will be prospectively collected at baseline, prior to cycle 2 of each arm, and at time of disease progression or the 12-month mark, whichever comes first for exploratory analyses including (1) immune and genomic profiling of liquid biopsies; (2) transcriptional profiling of baseline tumor biopsies; and (3) interrogation of the gut microbiome and bacterial functionality.
Up to 78 patients will be enrolled under the assumption of an improved 12-month PFS from 50% ipilimumab and nivolumab alone to 75% among those who receive ipilimumab and nivolumab plus SBRT, using a two-sided α = 0.1, power = 80%, and accounting for loss-to-follow-up and stratification using IMDC criteria 1-2 vs 3-6. The trial is currently enrolling in Canada and Australia.
Presented by: Aly-Khan A. Lalani, MD, FRCPC, Department of Oncology, Juravinski Cancer Centre, McMaster University, Hamilton, ON, Canada