(UroToday.com) The field of advanced prostate cancer has rapidly progressed over the past 15 years. Prior to publication of TAX-327, there were no proven life-prolonging therapies for patients with metastatic castration-resistant prostate cancer (mCRPC). Since that time, there have been many new agents that have proven survival benefits including taxane-based chemotherapy, agents targeting the androgen axis, and bone-targeting agents. In spite of castration resistance, mCRPC remains driven by activated androgen receptors and elevated intratumoral androgens. Thus, maximal androgen-axis targeting treatment may require dual inhibition of these two pathways. To this end, in a plenary abstract presentation in the Oral Abstract Session: Prostate Cancer session at the 2021 ASCO GU Cancers Symposium, Dr. Rathkopf presented results of the ACIS trial assessing the combination of apalutamide + abiraterone acetate (two approved prostate cancer treatment with distinct receptor inhibition and ligand suppression actions, respectively) as compared to abiraterone acetate alone in patients with chemo-naive mCRPC.
The authors accrued patients with mCRPC who had not received other life-prolonging therapy since diagnosis. In addition to ongoing androgen deprivation therapy (ADT), patients were randomized 1:1 to receive apalutamide (240 mg po QD) + abiraterone acetate (1000 mg po QD) + prednisone (5 mg po BID) or placebo + abiraterone acetate + prednisone (stratified by presence or absence of visceral metastases, Eastern Cooperative Oncology Group performance status 0 or 1, and geographic region). The primary endpoint was investigator-assessed rPFS (defined from randomization date to radiographic progression date or death). Additionally, the authors assessed other secondary endpoints including prostate-specific antigen (PSA) response, overall survival (OS), safety, time to PSA progression, chronic opioid use, initiation of cytotoxic chemotherapy, and pain progression.
Between December 2014 and August 2016, the authors enrolled 982 patients and followed them for analyses of both rPFS and OS.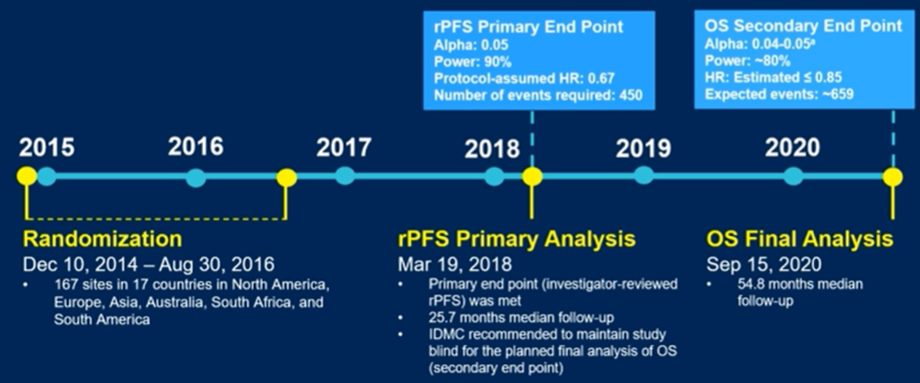
At baseline, the two arms were well balanced with respect to demographic and tumor characteristics.
Based on the pre-planned final analysis of rPFS in March 2018, treatment with apalutamide + abiraterone acetate was an associate with improved rPFS (22.6 months) compared to abiraterone acetate alone (16.6 months; hazard ratio 0.69 [95% CI 0.58-0.83]; p < 0.0001)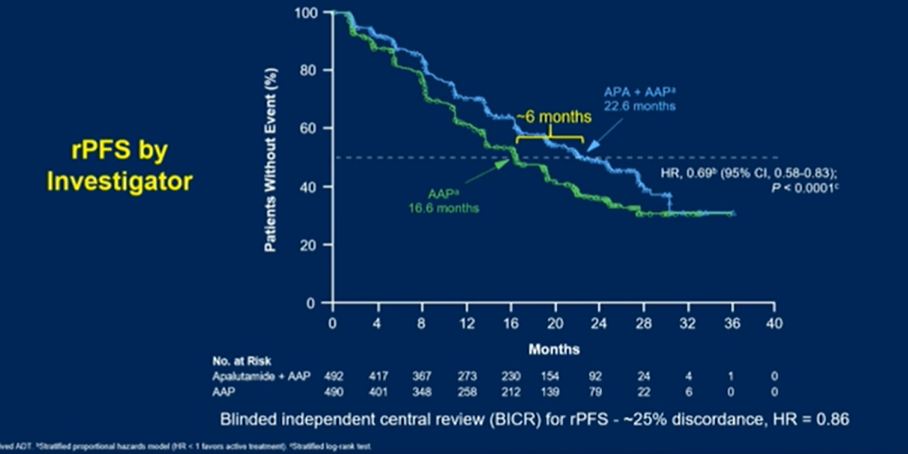
Pre-specified subgroup analyses demonstrated that the benefit of the combined approach was consistent across strata of performance status, visceral disease, geographic region, number of bony lesions, age, and PSA.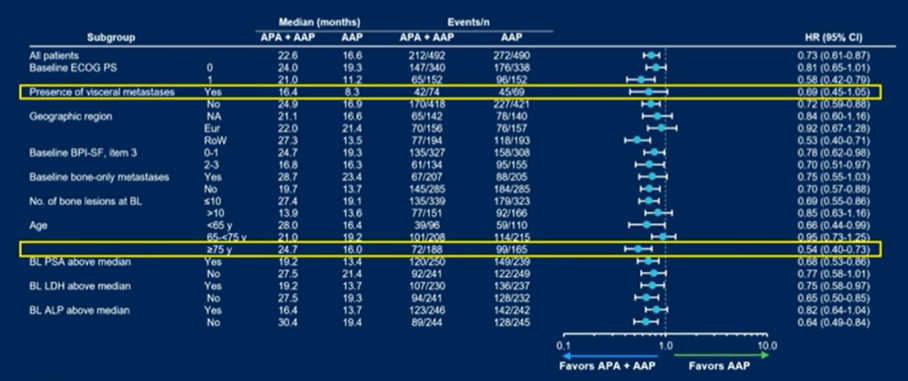
At the same time, representing the first interim analysis of overall survival at a median follow-up of 25.7 months, median overall survival was improved by 2.5 months though this was not statistically significant.
However, blinded follow-up continued. At the updated final analysis in September 2020, with a median follow-up of now 54.8 months, rPFS remained improved in patients receiving the combination approach (hazard ratio 0.70, 95% confidence interval 0.60 to 0.83) with 7.3 month improvement in median rPFS. However, at the updated final analysis, no improvement in overall survival was noted with a hazard ratio of 0.95 (95% confidence interval 0.81 to 1.11).
Other secondary endpoints including time to PSA progression, chronic opioid use, initiation of cytotoxic chemotherapy, and pain progression did not differ statistically significantly between arms.
However, PSA response rates were higher among patients receiving combination treatment. Unfortunately, this translated into only a marginal delay in PSA progression (13.8 vs 12.0 months, p=0.076).
In men who have historically had a particularly poor prognosis, namely those with visceral disease and older men, the combination approach was associated with apparent benefits in both rPFS and OS, although the statistical significance was marginal for many of these comparisons.
The use of biomarker selection with patients with PAM50 liminal and AR activity average or high appearing to derive greater benefit from the combination approach.
The majority of patients in this trial received subsequent life prolonging therapy with chemotherapy used in approximately 70% of patients in each arm.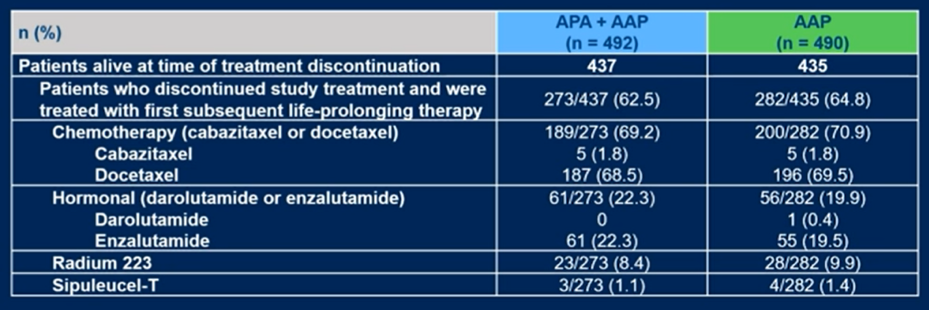
The combination of apalutamide + abiraterone acetate was not associated with any new safety signals: grade 3/4 treatment-emergent adverse events (TEAEs) were reported in 63.3% (310/490) of APA + AAP–treated pts vs 56.2% (275/489) of AAP-treated pts, with more grade 3 (56.1%, 275/490 vs 45.6%, 223/489) and less grade 4 (7.1%, 35/490 vs 10.6%, 52/489) TEAEs, respectively.
Additionally, the authors assessed health-related quality of life finding that this was comparable between the treatment groups.
The authors conclude that the ACIS trial met the primary endpoint of rPFS, demonstrating a 31% reduction in risk of radiographic progression or death in chemo-naive mCRPC patients treated with the combination of apalutamide + abiraterone acetate compared to abiraterone acetate alone, in combination with continued ADT.
Presented by: Dana E. Rathkopf, MD, Medical Oncologist, Memorial Sloan-Kettering Cancer Center
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center Contact: @WallisCJD on Twitter during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021