Dr. Valicenti began by summarizing the two studies he provided a discussion for, emphasizing that these data bring us closer to personalized treatment. In the two relevant presentations, the two talks examine whether post-operative PSA dynamics and conventional imaging can identify a benefit to dose-escalated salvage radiotherapy and how a combined clinical and cell-cycle risk score can be used to de-intensify treatment for patients with intermediate and high risk prostate cancer.
Summarizing the SAKK 09/10 randomized trial of conventional as compared to dose-intensified salvage radiotherapy, he concluded that the answer to the first question is a resounding no, with standard approaches unable to detect a dose-response in post-operative radiotherapy.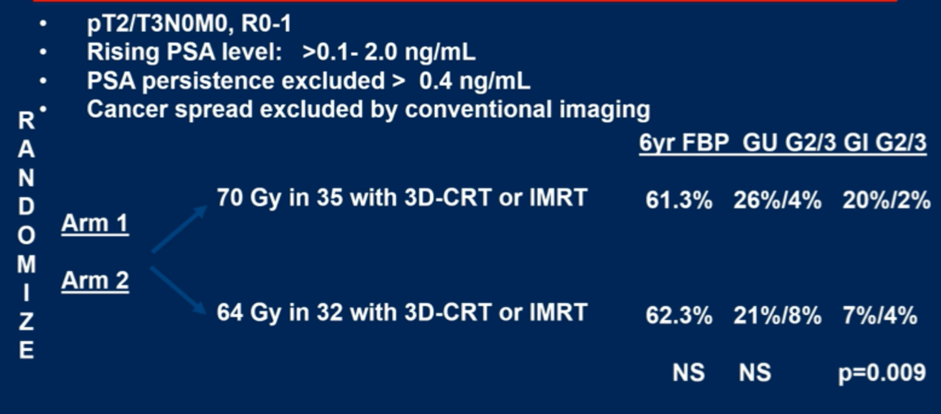
In spite of a lack of oncologic benefit, dose-intensification was associated with higher rates of gastrointestinal toxicity. These results are in line with prior data from Peking University. However, in contrast, among patients with an intact prostate, Dr. Valicenti highlighted that many randomized trials, including cooperative group trials, have demonstrated improvements in biochemical control with dose-escalation.
Given the intact prostate, all of these trials had a radiographically identifiable target, which differs from the two post-operative trials. Thus, Dr. Valicenti concludes that it is beneficial to have a targetable lesion for dose-escalation. He then highlighted data from the Falcon trial suggesting that the use of advanced imaging can provide actionable information to modify radiation planning.
Such targeting may also allow for improvements in biochemical control in men with biochemically-recurrent cancer.
Only recently, the EMPIRE-1 trial demonstrated, in a phase III trial, failure-free survival was improved by 24% at 4 years with radiotherapy targeting informed by advanced imaging, in this case fluciclovine-PET.
Dr. Valicenti then turned his attention to the presentation from Dr. Tward. He began by summarizing a number of cooperative group trials which have clearly demonstrated that the addition of ADT to radiotherapy, compared to radiotherapy alone, improves outcomes for men with intermediate- and high-risk prostate cancer.
Despite these trials, absolute risk reductions range from 2-12% at 10 years following randomization. Thus, there is a rationale for better prognostic markers to inform treatment decisions. This is particularly relevant as it relates to the use of concomitant ADT given both the nuisance and serious medical complications associated with its use.
Clinical and genomic classifiers may allow for estimation of individual risk to inform treatment decision making. In the presentation from Dr. Tward, the combined clinical and cell-cycle risk score was used in this context. They determined a threshold below which ADT could be safely withheld, given the low absolute risk of metastases. In particular, they identified that a CCR of 2.112 or less was associated with 10-year risk of metastasis of 4.1%, which varied very little whether ADT was administered (3.9%) or not (4.2%).
However, the ASCO guideline on molecular biomarkers in localized prostate cancer specifically comments that use of these assays is not recommended for routine clinical use given their lack of prospective testing and evidence of improvement in long-term outcomes. In Dr. Valicenti’s view, use of the CCR warrants testing in non-inferiority studies in which patients below the multimodality threshold are randomized to receive radiotherapy with or without androgen deprivation therapy. The NRG-GU009 is such a study utilizing Decipher for genomic risk stratification.
In conclusion, Dr. Valicenti concluded that PSA dynamics and conventional imaging are insufficient to individualize post-operative dose-intensification, though advanced imaging may allow the definition of patient-specific targets to allow for improvements. Further, genomic markers that allow for prognostication of the absolute risk of disease progression may allow for more personalized care but require prospective validation.
Presented by: Richard K. Valicenti, MD, MA, FASTRO, Chair and Professor of Radiation Oncology at the University of California Davis Comprehensive Cancer Center, UC Davis Health
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, @WallisCJD on Twitter during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021
Related Content:
ASCO GU 2021: Dose-Intensified Versus Conventional Dose-Salvage Radiotherapy for Biochemically Recurrent Prostate Cancer After Prostatectomy: Six-Year Outcomes of the SAKK 09/10 Randomized Phase III Trial
ASCO GU 2021: Association of the Clinical Cell-Cycle Risk Score with Metastasis After Radiation Therapy and Identification of Men with Prostate Cancer Who Can Forgo Combined ADT