The SAKK 09/10 trial (NCT01272050) is an open-label, multicenter, randomized Phase III trial performed in 24 centers in Switzerland, Germany, and Belgium. The authors recruited men with biochemical progression (two consecutive rises with the final prostate-specific antigen (PSA) > 0.1 ng/mL or three consecutive rises) after RP with a PSA nadir of ≤ 0.4 ng/mL, with a PSA ≤ 2 ng/mL at randomization. Further, patients had to have no evidence of macroscopic disease and no nodal involvement at radical prostatectomy.
Following enrollment, patients were randomly assigned to receive either conventional-dose RT (64 Gy in 32 fractions) or dose-intensified RT (70 Gy in 35 fractions) directed to the prostate bed. Both 3-dimensional conformal RT and intensity-modulated RT/rotational techniques were used. The authors assessed the primary endpoint of freedom from biochemical progression (PSA ≥ 0.4 ng/mL and rising), as well as secondary endpoints of clinical progression-free survival, time to hormonal treatment, overall survival, acute and late toxicity (according to the National Cancer Institute Common Terminology Criteria for Adverse Events [NCI CTCAE] v4.0) and quality of life (according to the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire [EORTC QLQ]-C30 and PR25).
Between February 2011 and April 2014, a total of 350 patients were randomly assigned to conventional-dose RT (64 Gy) (n = 175) or dose-intensified RT (70 Gy) (n = 175). Among these 350 patients, 344 patients (aged 48 to 75 years) were assessable for the intention-to-treat population.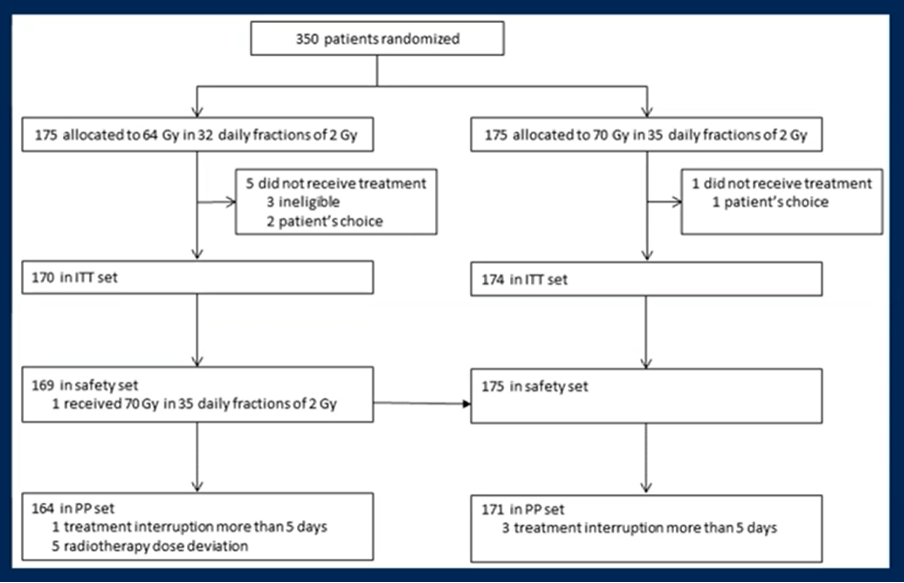
At the time of randomization, the median PSA was 0.3 ng/mL (range, 0.03-1.61 ng/mL), in keeping with relatively early salvage radiotherapy.
As of a data cut-off of July 3, 2020, the median follow-up was 6.2 years (IQR 5.5-7.2) and 138 biochemical progression events had occurred. The estimated 6-year freedom from biochemical progression was 62.3% (95% confidence interval [CI] 54.2-69.4%) among patients in the conventional dosage arm and 61.3% (95% CI 53.4-68.3%) among patients in the dose-intensified arm. After adjustment for stratification factors, there was no difference in freedom from biochemical progression (hazard ratio [HR] 1.14, 95% CI 0.82-1.60; log-rank p = 0.44).
This effect was consistent across subgroups.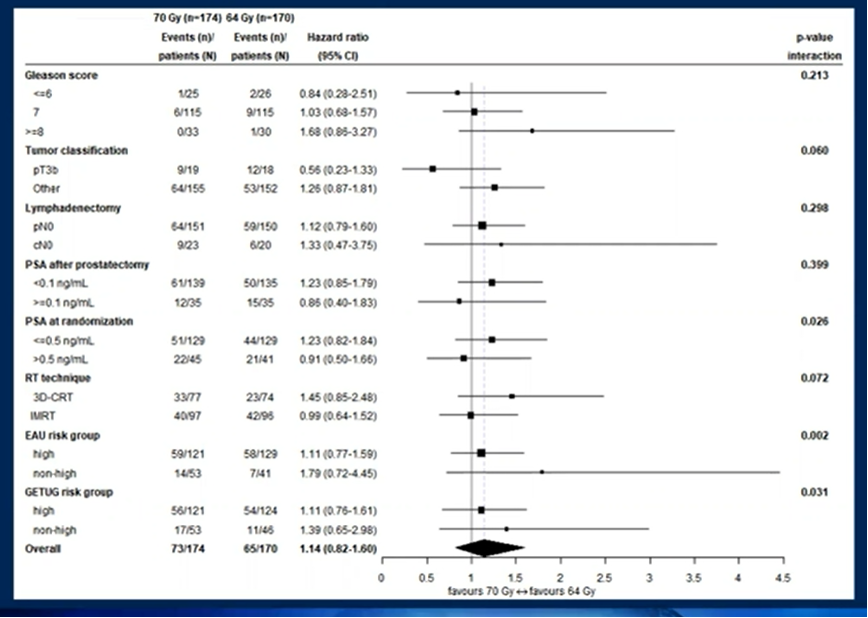
Assessing secondary efficacy endpoints, there were no significant differences found for clinical progression-free survival, time to hormonal treatment, and overall survival. In fact, Kaplan Meier survival curves for these outcomes were nearly entirely superimposed.
Similarly, rates of late grade 2 and 3 genitourinary toxicity did not significantly differ though late grade 2 and 3 gastrointestinal toxicity was more common in patients receiving dose-intensified RT (35 (20%) and 4 (2.3%) vs. 12 (7.3%) and 7 (4.2%); p=0.009). Assessing patient-reported quality of life, no differences were noted between the two arms.
The authors concluded that dose-intensification at the time of salvage radiotherapy is not associated with oncologic improvements but does have higher rates of late grade 2 and 3 gastrointestinal toxicity.
Presented by: Pirus Ghadjar, MD, Attending Physician, Department of Radiation Oncology, Charité Hospital, Berlin, Germany
Written by: Christopher J.D. Wallis, MD, PhD, Urologic Oncology Fellow, Vanderbilt University Medical Center, Nashville, Tennessee, Twitter: @WallisCJD during the 2021 ASCO Genitourinary Cancers Symposium (ASCO GU), February 11th to 13th, 2021