Dr. Gopalan states that although there is an improvement in prognostication with Gleason Grade groups, there is still heterogeneity with regards to Gleason 4, specifically the percentage of Gleason 4. Cole et al.1 assessed the prognostic value of Gleason 4 percentage in cancer-related outcomes of 1,691 men undergoing radical prostatectomy. Among these patients, 517 (30.6%) had adverse pathological features and 86 (5.6%) experienced biochemical recurrence. The following figure highlights the probability of adverse pathology and biochemical recurrence by Gleason pattern 4 percentage:
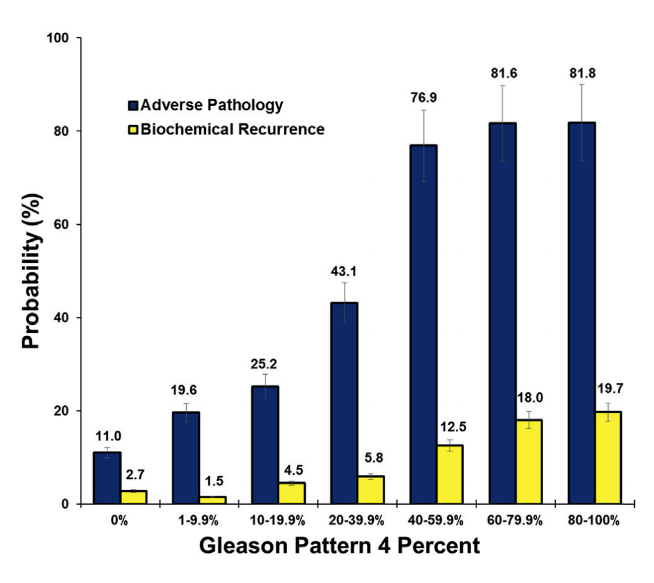
On multivariable analyses, Gleason 4 percentage was a significant predictor of adverse pathology (odds ratio [OR] 1.04, 95% confidence interval [CI] 1.03-1.05) and time to biochemical recurrence (hazard ratio [HR] 1.02, CI 1.01-1.03). Gleason 4 percentage was also a significant independent predictor of adverse pathology in subsets of patients with Gleason score 7 (OR 1.05, 95% CI 1.03-1.06), Gleason 3+4 (OR 1.06, 95% CI 1.04-1.08), and Gleason 4+3 cancer (OR 1.05, 95% CI 1.03-1.06). Additionally, this study found a significantly increased risk of adverse pathology at potentially meaningful Gleason 4 percentage thresholds (1% to 10% vs. 20% to 30%).
Additional work has been done assessing percent Gleason 4 and cribriform/intraductal carcinoma with the Decipher® genomic classifier assay. A study from the University of Michigan assessed whether the presence of cribriform, intraductal carcinoma, and percent Gleason 4 was associated with an increased genomic risk as measured by the Decipher® assay in a prospective cohort of 48 patients.2 They found that the presence of cribriform/intraductal carcinoma was significantly associated with Decipher® risk score (p = 0.007), with a high-risk Decipher® score in 22% vs. 56% of patients without or with cribriform/intraductal carcinoma. Additionally, percent Gleason 4 (OR 1.04 per percent increase, 95% CI 1.02-1.06) and cribriform predominant histology (OR 9.60, 95% CI 1.48-62.16) were significantly associated with a high-risk genomic classifier score, whereas intraductal carcinoma did not reach significance (OR 1.92, 95%CI 0.65-5.67).
Several retrospective studies have assessed the presence of DNA damage repair (DDR) mutations and the association with disease histology. Men with germline mutations are generally more likely to harbor intraductal histology (48% vs. 12%) than those without mutations, highlighting that high-risk patients (ie. those with cribriform/intraductal carcinoma) should be offered genetic screening based on the NCCN guidelines.
Dr. Gopalan concluded her presentation with the following take-home messages:
- Grade grouping and quantification of Gleason pattern 4 offer a nuanced addition for risk stratification
- Histological features such as cribriform and intraductal carcinoma are complementary to clinicopathologic and molecular data
- Biomarkers are important but are only robust if they give additive value to a base model incorporating standard clinical and pathologic variables as opposed to just associations
Presented by: Anuradha Gopalan, MD, Surgical Pathologist, Memorial Sloan Kettering Cancer Center, New York, New York
Written By: Zachary Klaassen, MD, MSc, Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Augusta, Georgia, Twitter: @zklaassen_md during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021
References:
1. Cole, Adam I., Todd M. Morgan, Daniel E. Spratt, Ganesh S. Palapattu, Chang He, Scott A. Tomlins, Alon Z. Weizer et al. "Prognostic value of percent Gleason grade 4 at prostate biopsy in predicting prostatectomy pathology and recurrence." The Journal of urology 196, no. 2 (2016): 405-411.
2. Taylor, Alexander S., Todd M. Morgan, David G. Wallington, Arul M. Chinnaiyan, Daniel E. Spratt, and Rohit Mehra. "Correlation between cribriform/intraductal prostatic adenocarcinoma and percent Gleason pattern 4 to a 22‐gene genomic classifier." The Prostate 80, no. 2 (2020): 146-152.