(UroToday.com) The treatment landscape for first-line therapy among patients with metastatic renal cell carcinoma (mRCC) has changed dramatically over the past 2 years. In 2018, the publication of the CheckMate214 data demonstrated a survival benefit for patients treated with nivolumab and ipilimumab compared with sunitinib in intermediate and poor-risk mRCC, ushering in the immunotherapy era for mRCC. The subsequent publication of the JAVELIN Renal 101, KEYNOTE-426, and CheckMate-9ER studies demonstrated the superiority of avelumab and axitinib, pembrolizumab and axitinib, and nivolumab and cabozantinib compared to sunitinib in this disease space. In a plenary abstract presentation in the Poster Highlights Session: Renal Cell Cancer - Clinical Trial Updates session at the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (ASCO GU), Dr. Plimack and colleagues provide an update on the KEYNOTE-426 study examining outcomes for patients who received pembrolizumab and axitinib and have completed two years of follow-up.
To briefly summarize the previously reported methodology of the study, patients included in KEYNOTE-426 had treatment naïve clear cell RCC and measurable disease (per RECIST v1.1). Patients were further required to have KPS ≥70%. Eligible patients were randomly assigned in a 1:1 fashion to receive pembrolizumab 200 mg intravenously every 3 weeks for up to 35 doses + axitinib 5 mg orally twice daily or sunitinib 50 mg once daily (4 weeks on/2 weeks off) until progression, toxicity, or withdrawal. 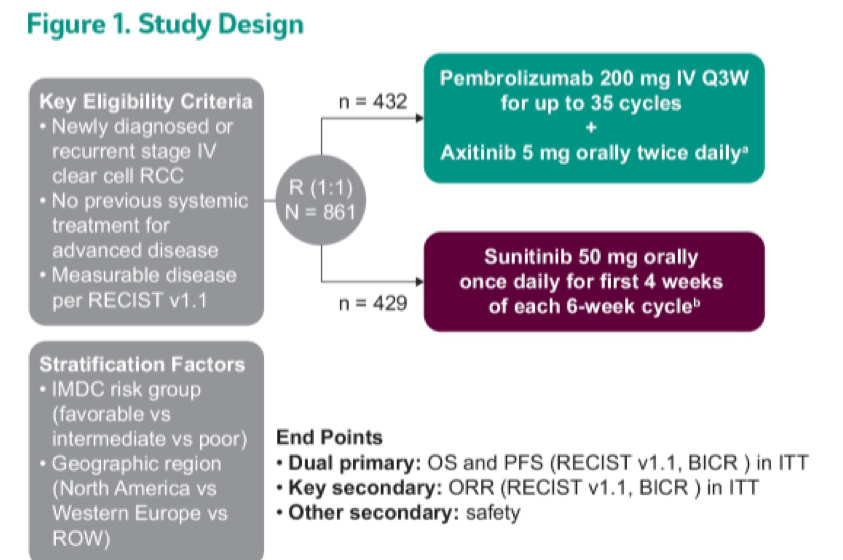
The primary end points were overall survival (OS) and progression-free survival (PFS), with key secondary end points of objective response rate (ORR) and safety. According to protocol, patients could discontinue pembrolizumab or axitinib and continue the other agent. Pembrolizumab was stopped for all patients at 2 years. Axitinib could be continued until progression or toxicity. In this presentation, the authors report an exploratory subgroup analysis of KEYNOTE-426 describing outcomes of patients who completed 2 years of pembrolizumab.
Among 432 patients who were treated with pembrolizumab and axitinib, 129 (29.9%) completed 2 years of study therapy. The authors further limited their analysis to 103 patients who didn’t discontinue axitinib due to progressive disease. The median (range) age of these patients was 61 (36-82) years, and 73.8% were male.
The majority of patients in this subset had International mRCC Database Consortium intermediate/poor risk disease (n=67) while 36 had favorable risk disease, consistent with the intention-to-treat population.
The median (range) follow-up duration from randomization to data cut-off was 30.1 (24.0-37.7) months. Among patients who completed 2 years of study therapy, neither median overall survival or median progression-free survival were reached as of 3 years.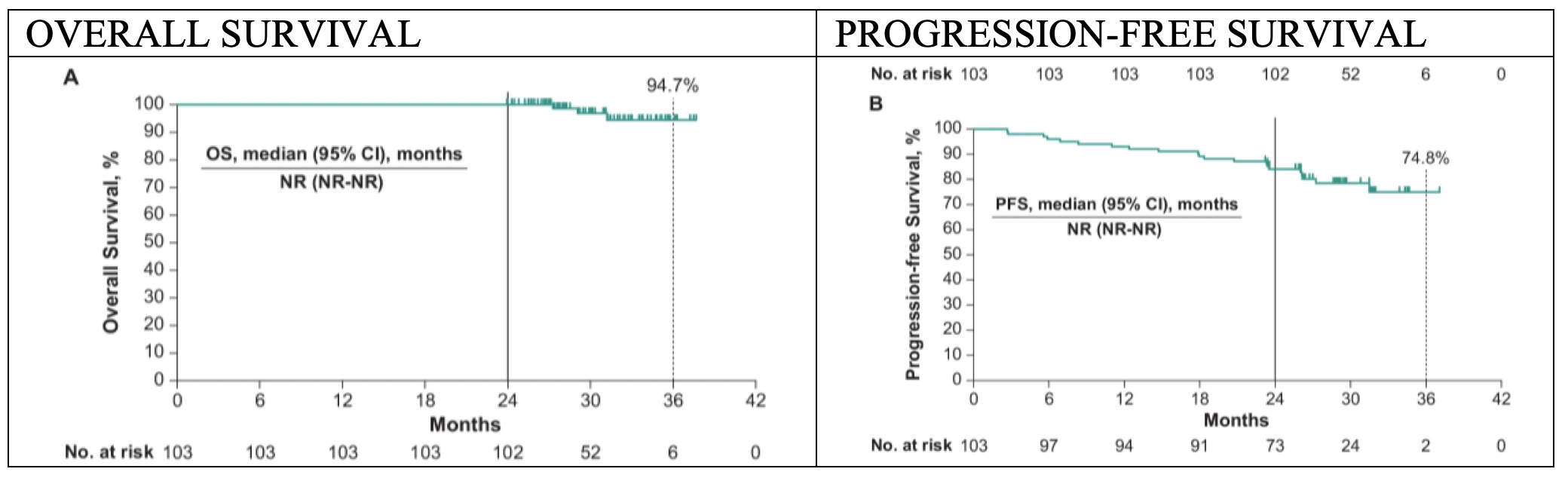
85.4% of patients who completed two years of therapy per protocol had objective response, of which 16 patients had complete response.
On multivariable analysis, patients younger than 65 years (OR 1.76, 95% CI 1.07-2.90), those with performance status of 90/100 (OR 2.10, 95% CI 1.03-4.24), those with favourable (OR 4.99, 95% CI 1.63-15.27) and intermediate (OR 4.90, 95% CI 1.67-14.41) risk disease, and those with sarcomatoid features (OR 2.19, 95% CI 1.08-4.43) were more likely to complete two years of therapy.
60.2% of patients experienced grade 3-4 treatment-related adverse events without any Grade 5 events.
The authors conclude that this exploratory analysis demonstrates that a significant proportion of patients in the pembrolizumab and axitinib arm are able to complete 2 years of pembrolizumab with ongoing clinical benefit.
Presented by: Elizabeth R. Plimack, MD, MS, Chief, Division of Genitourinary Medical Oncology, Professor, Department of Hematology/Oncology, Director, Genitourinary Clinical Research, Fox Chase Cancer Center
Co-Authors: Thomas Powles, Jens Bedke, Frédéric Pouliot, Viktor Stus, Tom Waddell, Rustem Gafanov, Dmitry Nosov, Boris Alekseev, Raymond S. McDermott, Maurice Markus, Sophie Tartas, Anna Kryzhanivska, Igor Bondarenko, Cezary Szczylik, Jianxin Lin, Rodolfo F. Perini, L. Rhoda Molife, Michael B. Atkins, Brian I. Rini
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, @WallisCJD on Twitter during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021