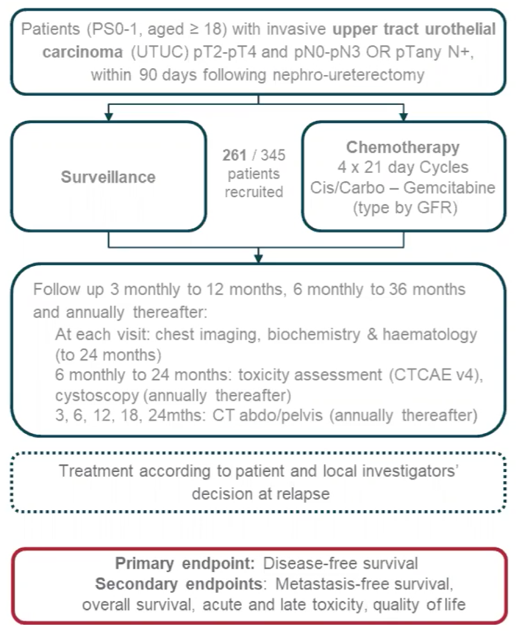
In POUT, 261 patients with upper tract urothelial carcinoma were enrolled following nephroureterectomy and randomized (1:1) to 4 cycles of gemcitabine-cisplatin (gemcitabine-carboplatin if GFR 30-49ml/min) or surveillance with subsequent chemotherapy if required. Patients had 6 monthly imaging and cystoscopy for 2 years, then annually to 5 years. The primary endpoint was disease free survival and secondary endpoints included metastasis free survival, overall survival, toxicity, and patient-reported quality of life. The trial was closed to recruitment early on the advice of the independent data monitoring committee due to evidence of efficacy. The trial schema for POUT is as follows:
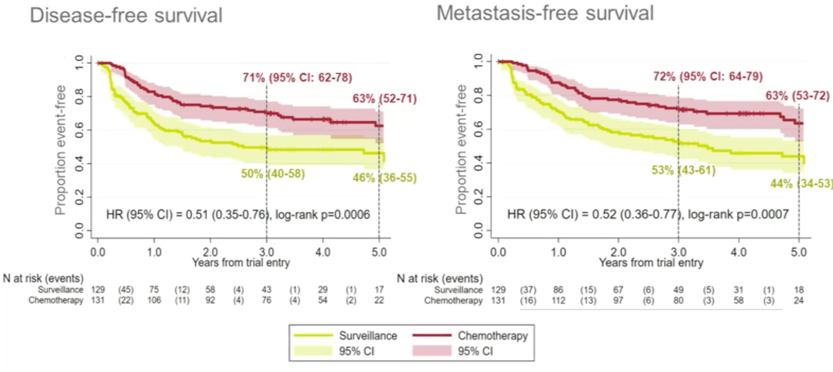
From May 2012 to November 2017, 261 patients were recruited (129 surveillance; 132 chemotherapy) at 56 UK centers. These patients had median age of 69 years (range 37-88), 28% were pT2, 66% were pT3, and 91% were pN0. Over a median follow-up of 48.1 months (IQR: 36.0-60.1), the unadjusted hazard ratios for disease free survival was 0.51 (95% CI 0.35-0.76; p = 0.0006) and for metastasis free survival was 0.52 (95% CI 0.36-0.77; p = 0.0007):
There were 93/260 (35.8%) patients that died (52/129 [40.3%] surveillance and 41/131 [31.3%] chemotherapy) during follow-up. Chemotherapy conferred a non-statistically significant 30% reduction in relative risk of death (HR 0.70, 95% CI 0.46-1.06; p = 0.09):

The 3-year overall survival rate for surveillance patients was 67% (95% CI 58-75%) and 79% for chemotherapy (95% CI 71%-86%). There was no evidence of long-term toxicity associated with chemotherapy, and the most common grade 2+ adverse events were hypertension (10.4%), lethargy (10.4%), and hearing loss (5.4%). There was no evidence of statistically or clinically relevant differences in quality of life 12 months after treatment (EORTC Q30 global health status mean difference 4.1 and 4.8 at 12 and 24 months, respectively, in favor of chemotherapy).
Dr. Birtle concluded her updated analysis of the POUT phase III trial with the following conclusions:
- The benefit of adjuvant chemotherapy on disease-free and metastasis-free survival was maintained with additional follow-up
- There was a non-statistically significant improvement in overall survival
- These updated analyses support the use of platinum-based adjuvant chemotherapy as a recommended standard of care
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021
References:
- Birtle A, Johnson M, Chester J, et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): A phase 3, open-label, randomized controlled trial. Lancet 2020 Apr 18;395(10232):1268-1277.