(UroToday.com) Cisplatin chemotherapy is the standard of care for medically fit patients in advanced urothelial carcinoma. Up to 50% of these patients are medically ineligible for cisplatin due to low performance status, renal dysfunction, or other medical comorbidities. Immune checkpoint blockade is a first line therapeutic option in either platinum ineligible patients or carboplatin eligible patients whose tumors also express PD-L1. Patients who are ineligible for cisplatin and progress on immune checkpoint blockade have limited treatment options, and many efforts are underway to expand the therapeutic armamentarium for this disease context.
Enfortumab vedotin (EV) is an antibody-drug conjugate therapeutic with promising efficacy in locally advanced or metastatic urothelial carcinoma. It consists of an antibody against Nectin-4, a protein highly expressed on the surface of most urothelial carcinoma. This antibody is conjugated to the anti-microtubule agent Monomethyl auristate E. Once the antibody binds the Nectin-4 expressing cell, the agent is internalized, and the chemotherapy agent is released to cause eventual cell death, as illustrated below. 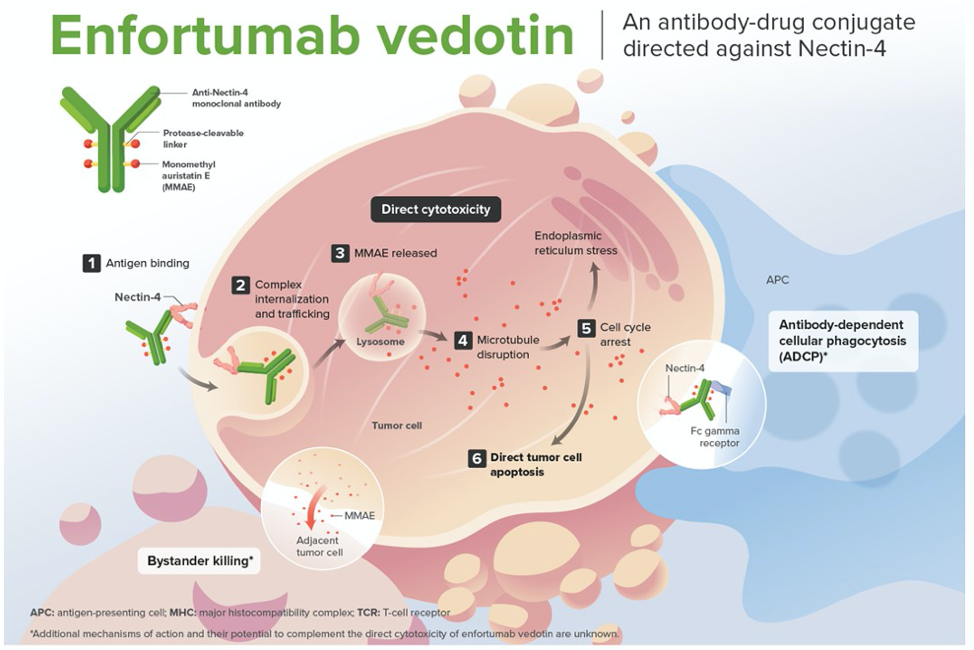
The EV-301 study was designed to confirm the benefit of EV for the treatment of patients with advanced urothelial carcinoma who have progressed after platinum chemotherapy and immune checkpoint blockade. The trial schema is shown below. The primary endpoint of the study was overall survival. Two analyses were planned, and interim analysis at 285 deaths of the estimated 600 patients to be enrolled, and a final analysis at 439 death.

In this presentation, Dr. Powles presented the results of the planned interim analysis. Patient characteristics were balanced between the chemotherapy and EV groups. The average age in both was 68 years, and patients were mostly men with Bellmunt risk score of 0-1. Approximately 30% of patients in each group had liver metastases, and around 20% of patients in each group had responded to prior immune checkpoint inhibition. In the EV arm, 134 patients had died, and 167 patients in the chemotherapy arm had died. The median duration of EV treatment was 5.0 months as opposed to 3.5 months of chemotherapy. Median follow-up was 11.1 months. Most patients discontinued treatment due to progressive disease, with ~15% of patients in each arm experiencing an adverse event that caused treatment discontinuation.
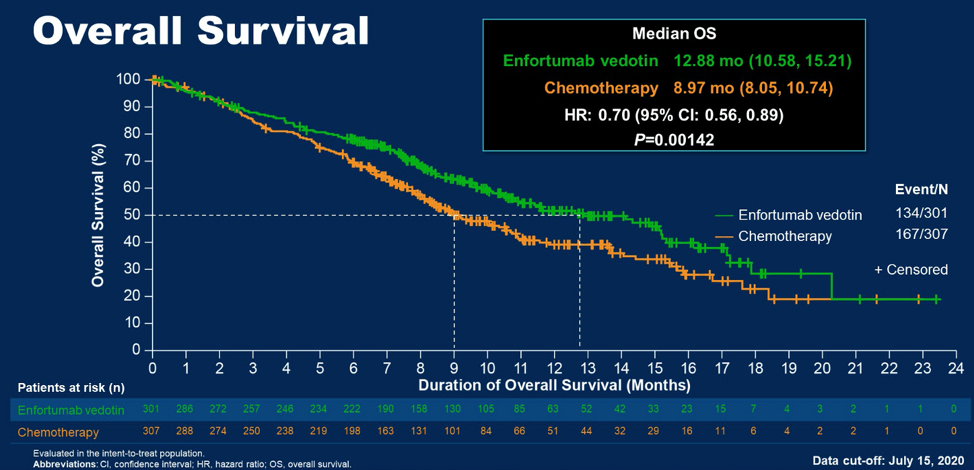
With regards to the primary endpoint, EV treatment was associated with a statistically significant improvement in overall survival relative to chemotherapy. The median overall survival in the EV group was 12.88 months as opposed to 8.97 months with chemotherapy, conferring a hazard ratio for death of 0.70 (95% CI 0.56 – 0.89, p = 0.00142) for EV therapy.
Subgroup analyses generally favored EV over chemotherapy. EV also conferred a statistically significant benefit for progression free survival of 1.8 months (HR 0.62, p < 0.0001). Almost 41% of patients had an overall response on EV therapy, with 5% complete responses, as opposed to 17.9% of patients receiving chemotherapy who had an overall response.
Notable differences in side effects for EV included more maculopapular rash (16% all grade, 7% grade 3+), less neutropenia and leukopenia, and lower incidence of febrile neutropenia (1% versus 6% in the chemotherapy arm). Adverse events of special interest for EV are shown below as compared to the chemotherapy group.
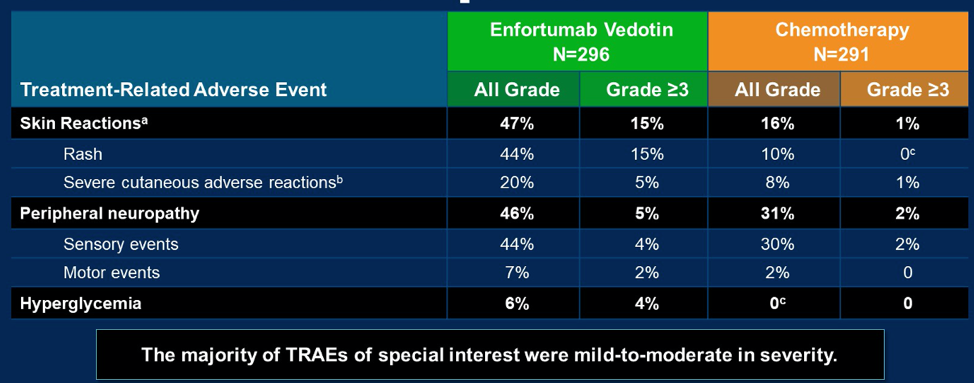
Dr. Powles concluded that the data presented confirm an overall survival advantage for enfortumab vedotin over chemotherapy for the treatment of patients with advanced urothelial carcinoma who have progressed on platinum chemotherapy and immune checkpoint blockade, consistent with earlier phase studies. Treatment-related events specific to EV, including neuropathy, skin reactions, and hyperglycemia were generally mild to moderate and manageable. The companion manuscript to this presentation has been simultaneously published in the New England Journal of Medicine.
Presented by: Thomas Powles, MBBS, MRCP, MD, Professor of Genitourinary Oncology, Lead for Solid Tumour Research at Barts Cancer Institute, Director of Barts Cancer Institute, London, United Kingdom
Written by: Alok Tewari, MD, PhD, Medical Oncologist at the Dana-Farber Cancer Institute, during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021
Related Content:
Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma