(UroToday.com) At the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (ASCO GU) session on optimizing personalized management of non-muscle invasive bladder cancer included a debate regarding the optimal therapy for BCG-unresponsive disease among patients that are not cystectomy candidates. Dr. Arjun Balar from NYU in New York made the argument for systemic therapy as the optimal treatment.
Dr. Balar notes that high-risk non-muscle invasive bladder cancer is a disease of systemic potential in need of systemic therapy. High-risk non-muscle-invasive bladder cancer is either CIS or high-grade Ta/T1, with TURBT and intravesical BCG the first-line standard of care. Although there is a complete response rate of 70% to initial intravesical BCG, most will not maintain the response, with 30% of patients experiencing recurrence within 1 year, 40% of patients at high risk of progressing to muscle-invasive disease, and 20-30% of patients progressing to metastatic disease. For BCG-unresponsive disease, the standard of care is radical cystectomy, which although is a morbid procedure, is justified.
According to Dr. Balar, there are several advantages to a systemic approach:
- Hitting the target – this is particularly relevant for treatment with a biological mechanism of action where key components of the treatment response are heterogeneously distributed
- Hitting the tumor – systemic therapy ensures clinical and subclinical (microinvasive and micrometastatic) disease is treated
- More reliable response assessment – current standard intravesical therapy (especially in the BCG-unresponsive setting) is luminally active, and “complete responses” may be entirely unreliable. Furthermore, complete responses (in particular to biological therapy) are more reliable with systemic therapy
Dr. Balar notes that at this meeting extended follow-up of KEYNOTE-057 was presented in which pembrolizumab was given to patients with high-risk non-muscle-invasive bladder unresponsive to Bacillus Calmette-Guerin. The trial design for KEYNOTE-057 is as follows:
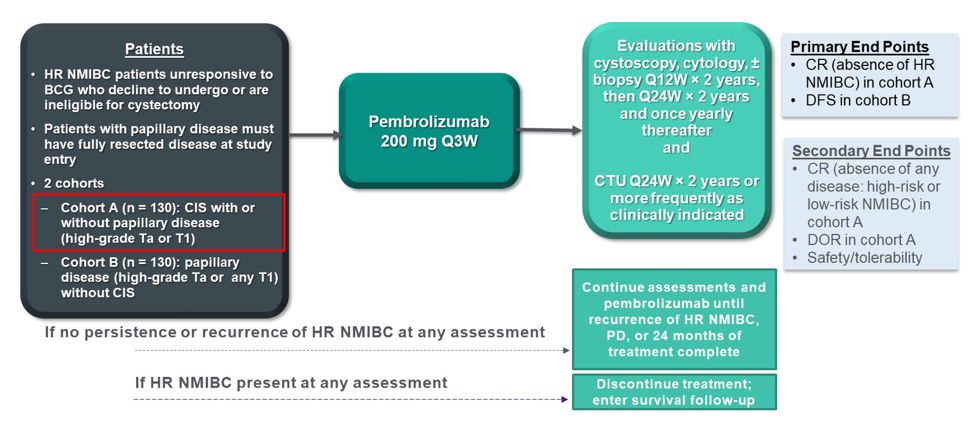
KEYNOTE-057 enrolled patients aged ≥18 years with histologically confirmed BCG–unresponsive high-risk carcinoma in situ, with or without papillary tumors, who were ineligible for or declined radical cystectomy to receive pembrolizumab 200 mg Q3W for up to 24 months or until disease persistence, recurrence, progression, or unacceptable toxicity. The primary endpoint for this trial was complete response rate, and key secondary end points included duration of response and safety. Overall, 101 patients received pembrolizumab and 96 were included in the efficacy analysis (5 patients did not meet BCG-unresponsive criteria). The median age of patients was 73 years (range: 44-92), and patients received a median of 12.0 (range: 7.0-45.0) BCG instillations. The primary endpoint of complete response at 3 months was met in 40.6% (95% CI 30.7-51.1) of patients. In the updated analysis, the median time from enrollment to data cutoff date of May 25, 2020, was 36.4 months (range: 26.3-48.5). Of 96 patients, the complete response rate was 40.6% (95% CI 30.7-51.1) at first evaluable disease assessment, and the median duration of response was 16.2 months (range: 0.0+ to 36.2). Among 39 responders, 13 (33.3%) remained incomplete response ≥18 months and 9 (23.1%) remained incomplete response ≥24 months. Dr. Balar notes that there are some toxicity concerns with systemic immunotherapy, however the majority will tolerate the treatment well and severe and irreversible immune-related adverse events are uncommon. Additionally, pembrolizumab delays cystectomy and, in data presented at this meeting, does not increase the risk of disease progression. There were 40 patients (41.7%) that underwent radical cystectomy after discontinuation of pembrolizumab: 35 pts (88%) had no pathologic upstaging to muscle-invasive bladder cancer, 2 (5%) had no available pathology data, and 3 (8%) had evidence of muscle-invasive bladder cancer (all non-responders):
Dr. Balar concluded is presentation highlighting that systemic therapy should be the treatment of choice for BCG-unresponsive NMIBC with the following take-home messages:
- Anti-PD-1 blockade induces complete responses in BCG-unresponsive CIS, which suggests systemic activation of anti-tumor activity
- Approval of pembrolizumab has redefined multidisciplinary care whereby the existing model is sequential in that a referral is made to medical oncology for chemotherapy and the patient then goes back to urology for a cystectomy. A future model will need to be shared/co-management in parallel to minimize safety risks
- Biomarkers remain a critical unmet need, with even greater clinical importance since cystectomy is highly curative
Presented by: Arjun V. Balar, MD, Perlmutter Cancer Center, NYU Langone Health, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021
Related Content:
Read the Opposing Debate: ASCO GU 2021: Optimal Therapy for BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer in the Non-cystectomy Candidate - Intravesical