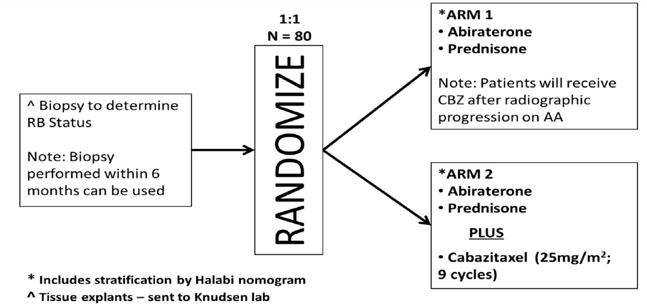
This is a multicenter non-comparative randomized Phase II trial in which patients were randomized 1:1 to abiraterone + prednisone with crossover to cabazitaxel upon abiraterone + prednisone failure (Arm 1), or the combination of abiraterone + prednisone + cabazitaxel (Arm 2). Randomization was stratified by the CALGB 90401 prognostic risk groups, and the primary endpoint was rPFS (time from randomization to radiographic progression or death, whichever occurs first). The trial schema is as follows:
Between October 2014 and March 2019, there were 93 patients accrued for this trial, of which 81 were randomized, including 42 to Arm 1 and 39 to Arm 2. The median age was 68.0 years (IQR 61.0-72.0) and ECOG performance status was 0 or 1. The trial endpoints were as follows:
- rPFS: Arm 1 median 7.9 months (95% CI 4.6-12.3) vs Arm 2 14.4 months (95% CI 10.4-20.5)
- rPFS hazard ratio (HR): Arm 1 0.5 (95% confidence interval [CI] 0.3-0.8) vs Arm 2 0.5 (95% CI 0.3-0.9)
- PFS progression: Arm 1 9.0 months (95% CI 6.4-13.4) vs Arm 2 13.8 months (10.7-17.6)
- Overall survival: Arm 1 16.4 months (95% CI 13.0-NR) vs Arm 2 20.7 months (12.8-NR)
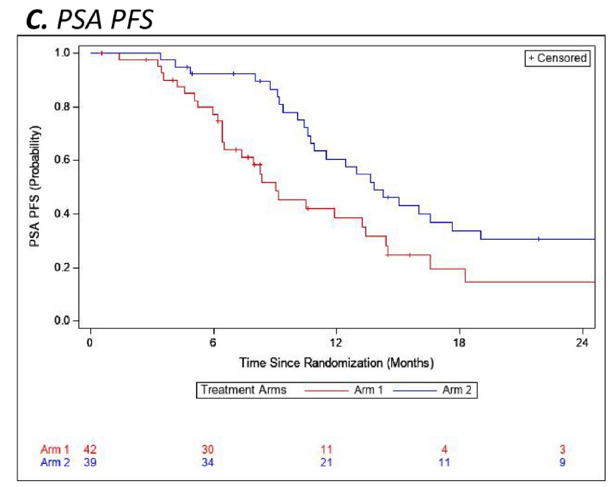
- ≥50% prostate-specific antigen (PSA) decline from baseline: Arm 1 52.4% (95% CI 36%-68%) vs Arm 2 87.2% (95% CI 73%-96%)
The Kaplan-Meier curves for rPFS, overall survival (OS), PSA, and progression-free survival (PFS) are as follows: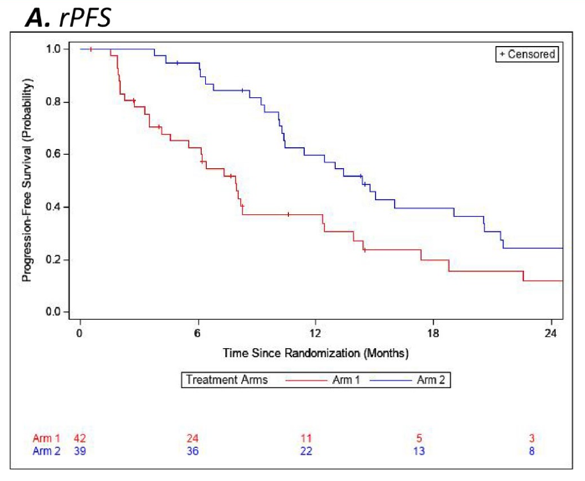

Dr. Slovin concluded the presentation of this trial with the following summary statements:
- Results of abiraterone + prednisone + cabazitaxel in chemotherapy-naïve patients suggest that men may derive benefit from the earlier use of cabazitaxel with acceptable toxicity, supporting further study of this combination in mCRPC patients
- Circulating Tumor Cells are being analyzed for changes in RB/AR expression.
Clinical trial information: NCT02218606
Presented by: Susan Slovin, MD, PhD, Associate Chair, Academic Administration, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York
Co-Authors: Karen E. Knudsen, Susan Halabi, Mark T. Fleming, Ana M. Molina, Steven Paul Wolf, Renee de Leeuw, Celina Fernandez, Praneet Kang, Traci Southwell, Carol L. Jones, Escarleth Fernandez, William Kevin Kelly; Memorial Sloan Kettering Cancer Center, New York, NY; Sidney Kimmel Cancer Center at Jefferson University, Philadelphia, PA; Duke University Medical Center, Durham, NC; Virginia Oncology Associates, US Oncology Research, Norfolk, VA; Weill Cornell Medicine, New York, NY; Duke University School of Medicine, Durham, NC; University of Illinois at Chicago, College of Medicine, Department of Pathology, Chicago, IL; Memorial Sloan-Kettering Cancer Center, New York, NY; Thomas Jefferson University, Philadelphia, PA; Virginia Oncology Associates, Norfolk, VA; Sidney Kimmel Cancer Center at Thomas Jefferson University, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California