Active surveillance is a preferred form of management for low risk prostate cancer. It is endorsed by multiple professional medical societies, and its implementation, although increasing, is still variable. There is still some concern among patients and providers that conventional assessment schemes miss a potion of clinically significant prostate cancer. However, the recent advances in imaging tools, biomarkers, and artificial intelligence are potential solutions to improve the risk stratification of these patients.
Some of the novel tools in the active surveillance risk assessment include germline analysis, integration of liquid biomarkers with imaging, and new imaging modalities such as micro ultrasound and PSMA PET scans. In the field of precision evaluation of localised disease, new tools have been assessed such as molecular imaging, image guided genetic cancer profiling, and machine learning or artificial intelligence for prediction of progression, staging and treatment.
There are also studies done on the impact of diet, exercise, and other lifestyle changes to reduce the risk of prostate cancer. There is a role for innocuous drugs such as statins, biguanides, 5 alpha reductase inhibitors and others. The impact of race, DNA repair and microsatellite instability (MSI) mutations, and other risk associated germline alleles is being studied.
Recently, a study assessing the effect of germline mutations in ATM and BRCA 1 and 2 on the rate of reclassification in men on active surveillance had been published1. The study included 1211 men on active surveillance of which 26 were with DNA repair germline mutations. These 26 men had a hazard ratio of 2 for any upgrading and specifically in men with BRCA2, their hazard ratio increased to 2.7 for any upgrading. Therefore, it is most likely not prudent to recommend active surveillance from men with germline mutations, especially those with BRCA2.
Genetic testing for inherited DNA repair defects has become inexpensive and widely available. There are many commercial assets available such as Color, Quest, Myriad, Ambry genetics, and Gene DX. The cost is as low as 100 to $250 and most can be easily and safely be performed at home. There is also the prostate genetic score (PGS), which incorporates genotype of over 30 prostate cancers associated SNPs . It uses weighted odd ratios of individualised SNPs. It has a sensitivity for metastatic disease of 94% and a negative predicted value of 97% for aggressive cancer. It is the only SNP based prostate cancer risk stratification tool currently available.
Dr. Klotz also mentioned the Pass Risk Calculator. This is a risk of classification based on individual patient factors. It is dynamic and may change overtime and the online interface provides clinical context, measure of model confidence, individual risk relative to the cohort, clinical consequences, and patient centered results.
The next topic discussed by Dr. Klotz was the use of MRI and biomarkers instead of biopsy. More data keeps coming in showing that eventually prostate MRI and biomarkers will replace the biopsy but we are not there yet. Both biomarkers and the MRI have known limitations that need to be acknowledged. It is important to understand the different clinical scenarios have varying needs. There is no doubt, that MRI is a game changer but it has important limitations. It is not a real time examination, It requires a radiologist, and a considerable learning curve. There are significant limitations to MRI in the post biopsy and post treatment setting. The MRI may miss small satellite lesions and underestimate legion volume, posing a challenge for focal therapy targeting. Additionally, there are issues of cost, complexity, patient anxiety and inconvenience. The MRI exclusions need to be taken into account as well. These including hip implants, claustrophobia and pacemakers.
Despite its limitations, there have been many studies assessing the MRI detection rate and ruling out of clinically significant cancer and these numbers are quite high (Table 1).
Table 1 - MRI detection rate and ruling out clinically significant cancer:
There is no doubt that MRI can replace some biopsies when utilising risk stratification. Overall, 15% of patients with negative MRI have clinically significant cancer on systematic biopsy and we need to remember this. Therefore, we should be aware of negative MRIs with significant risk factors such as high PSA density and high volume Gleason grade, and not abstain from biopysying these patients.
Next Dr. Kotz described the introduction of a high resolution micro ultrasound which could also be a game changer. This is the 29 MHz exact view micro ultrasound, which is considerably better than the conventional 6-9 MHZ ultrasound.It's resolution is up to 70 microns and it has a similar footprint and cost as a conventional ultrasound. It is now commercially available and has a very short learning curve. It uses its own scoring system which is called PRIMUS = Prostate risk identification using micro ultrasound (Figure 1). In an analysis comparing the metrics of micro ultrasound versus MRI using pooled analysis from 9 centres with almost 900 patients, the results showed that the micro ultrasound was at least as good as if not superior to MRI (Table 2).The current caveats of the micro ultrasound system include the fact that the data is still preliminary with only 1700 patients examined with this technology so far. Furthermore, the specificity and positive predictive value for this test are still unclear and the PRIMUS scoring system requires validation and updating.
Figure 1 – Micro US scoring system (PRIMUS):
Table 2 – Comparison of metrics of micro US vs. MRI: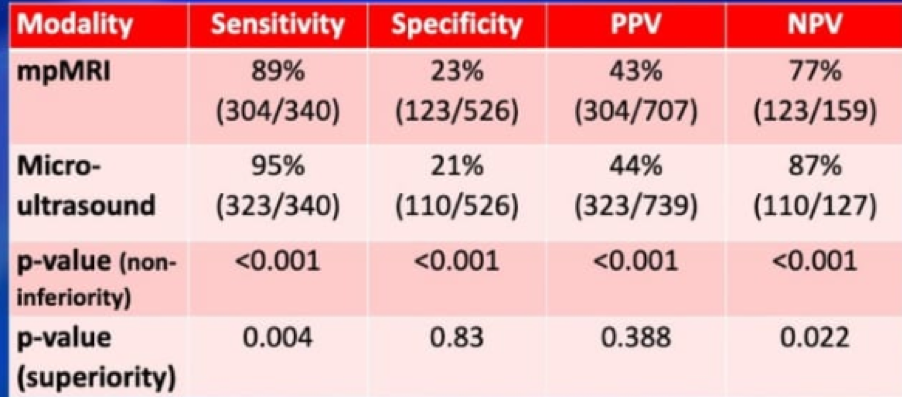
Dr. Klotz concluded his excellent talk discussing the advantages and disadvantages of the use of MRI and bimarker instead of a biopsy (Table 3) and there are several available biomarkers to date (Table 4). The genomic biomarkers add information to cancer grade, stage and PSA. An adverse genomic profile should promt reassessment or close follow-up, not immediate treatment. These genomic tests are optional for low risk and favourable intermediate risk disease. The genomic signature appears stable over time and further trials are underway. The current NCCN guidelines recommend incorporate genomic testing in the following patients (Table 5).
Table 3 – MRI or biomarker?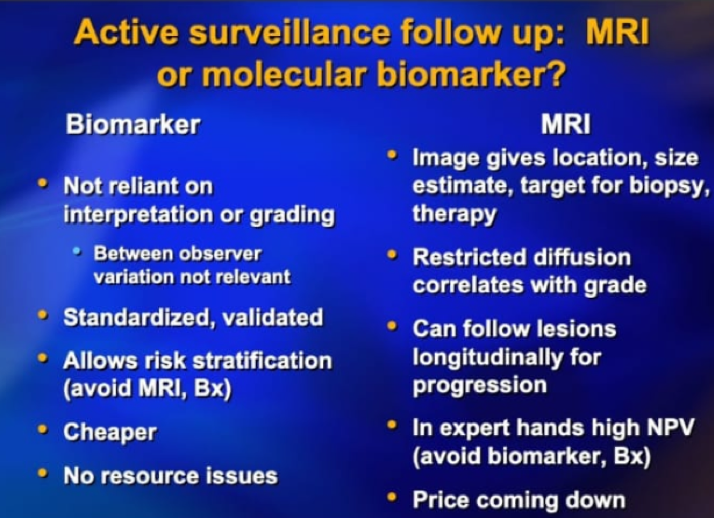
Table 4 - Available biomarker tests for significant prostate cancer:
Table 5 - Genomic testing acording to the NCCN guidelines:
Presented by: Laurence Klotz, MD, FRCSC, Sunnybrook Health Sciences Centre, Odette Cancer Centre, University of Toronto, Toronto, Ontario, Canada
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, NY, USA, @GoldbergHanan at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California
References:
1. Carter HB, Helfand B, Mamawala M, et al. Germline Mutations in ATM and BRCA1/2 Are Associated with Grade Reclassification in Men on Active Surveillance for Prostate Cancer. Eur Urol 2019; 75(5): 743-9.