San Francisco, California (UroToday.com) Neuroendocrine prostate cancer (NEPC) is a resistance-phenotype that emerges in men with metastatic castration-resistant prostate cancer (mCRPC) under the selective pressure of intense androgen receptor (AR) targeted therapy. NEPC is believed to emerge clonally from prostate adenocarcinoma (PRAD), retaining the original alterations seen in PRAD and gaining new alterations, both genetic and epigenetic. The timing of genetic and epigenetic events are not well understood. Obtaining repeat metastatic biopsies to understand tumor evolution is challenging. Circulating tumor DNA (ctDNA) may overcome some of these challenges as the collection is non-invasive, facilitating serial sampling.
In this session, Dr. Himisha Beltran, Associate Professor and Medical Oncologist at Dana-Farber Cancer Institute/Harvard Medical School, discussed the results of genetic and epigenetic profiling of paired tumor and ctDNA profiling from men with CRPC-PRAD and CRPC-NE. 62 men were included; the median PSA was 0.58 ng/ml.
Specific questions evaluated in this study were:
- Is circulating tumor DNA reflective of what we see in tumor biopsies (applying combined genomic/epigenomic classifier could pave the way for non-invasive detection of CRPC-NE)?
- What degree of heterogeneity underlies CRPC-NE compared with CRPC-PRAD?
- Can ctDNA distinguish clonal evolution/trans-differentiation versus rare clone selection?
Initially, the investigators found that there was no association between cfDNA content and pathologic subtype (PRAD or NEPC), site or number of metastases, serum PSA, or NEPC markers. Known genetic alterations that define CRPC-PRAD (i.e. AR gain of function) and CRPC-NE (loss of RB1 and TP53) were observed in ctDNA. Further, genetic alterations detected in ctDNA carried important prognostic information. AR gain was associated with worse outcomes in CRPC-PRAD, but not CRPC-NE. In contrast, loss-of-function alterations in ATM, BRCA1, and BRCA2 in ctDNA were associated with worse outcomes in both CRPC-PRAD as well as CRPC-NE.
An important question is a degree to which findings in ctDNA recapitulates tumor. Whole exome sequencing of paired ctDNA and tissue biopsies showed high concordance. Interestingly, there was less intra- and inter-patient heterogeneity in CRPC-NE than CRPC-PRAD. In an informative analysis, the investigators performed a serial sampling of ctDNA from two patients: one who was “AR driven” and one who was “AR independent”. Notably, in the AR driven patient, there was significant heterogeneity across temporal samples, suggesting that there are multiple clones competing with dynamic changes over time as measured by ctDNA shed. In contrast, in the AR independent patient, the same set of genetic alterations are present at different time points, suggesting that there is a single dominant clone that persists over time.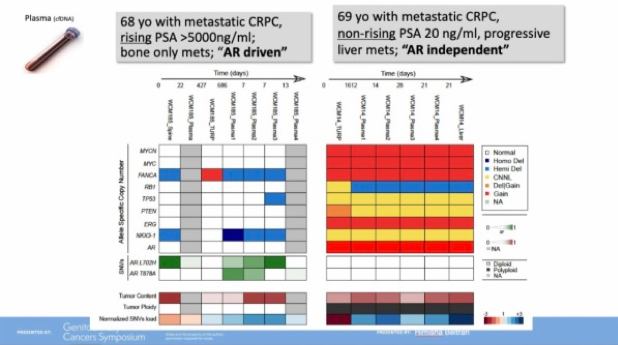
Whole-genome bisulfite sequencing of cell-free DNA identified known sites of differential methylation between CRPC-PRAD and CRPC-NE samples based on previous tissue methylation analysis. Specific sites, shown below, demonstrate concordance between locus specific methylation in both ctDNA and tissue.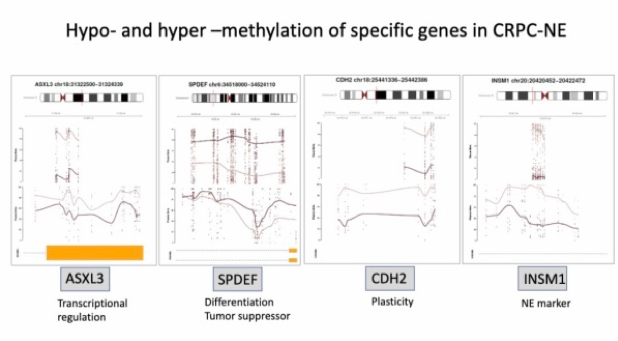
Finally, the investigators determined that a previously-derived genomic-methylation combined score distinguished CRPC-NE from CRPC-PRAD in ctDNA.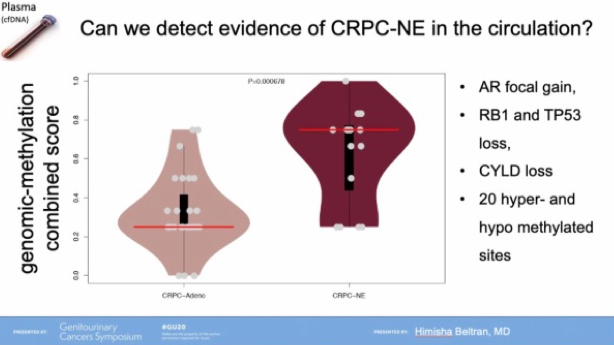
Dr. Beltran concluded with open questions that remain to be answered:
- How often and when does CRPC-NE emerge post-potent AR therapy?
- Are there high-risk localized or metastatic patients with CRPC-NE alterations?
- Does RB! +/- TP53 genomic loss or other features predispose patients to future neuroendocrine transformation? What else is needed to develop histologic transformation?
- When are emerging targets for NEPC (eg BRN2, MYCN, DLL3) expressed?
- How can we develop liquid biopsies for clinical trial selection?
Presented by: Himisha Beltran, MD, Associate Professor, and Medical Oncologist at Dana-Farber Cancer Institute/Harvard Medical School
Written by: Jacob Berchuck, MD, Medical Oncology Fellow at the Dana-Farber Cancer Institute (Twitter: @jberchuck) at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California