The first trial Dr. Ost discussed was the trial of ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-prostate cancer randomized, non-inferiority, Phase III trial.1 The Scandinavian HYPO-RT-PC randomized controlled Phase III trial was initially presented at ESTRO 2018 and was subsequently published in Lancet Oncology. This trial randomized men with intermediate and high-risk prostate cancer to either conventional fractionating (n = 602; 78.0 Gy in 39 fractions, 5 days per week for 8 weeks) or ultrahypofractionated (n=598; 42.7 Gy in seven fractions, 3 days per week for 2.5 weeks).
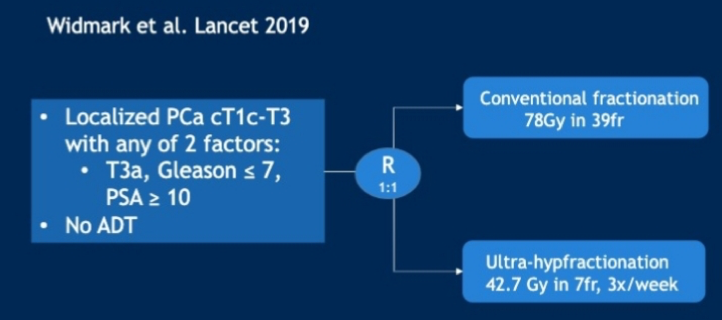
The primary endpoint was time to biochemical or clinical failure. The estimated failure-free survival at five years was 84% (95% confidence interval [CI] 80-87) in both treatment groups, with an adjusted hazard ration (HR) of 1.002 (95% CI 0.758-1.325; log-rank p=0.99). There was weak evidence of an increased frequency of acute physician-reported RTOG grade 2 or worse urinary toxicity in the ultra-hypofractionation group at end of radiotherapy (158 [28%] of 569 patients vs 132 [23%] of 578 patients; p=0.057). Based on these results, there has been support for the use of ultra-hypofractionated radiotherapy for prostate cancer.
The second trial Dr. Ost presented was the intensity-modulated fractionated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B) trial assessing acute toxicity from an international, randomized, open-label, Phase III, non-inferiority trial.2 Patients were either low-risk or intermediate-risk prostate adenocarcinoma (Gleason 4 + 3 excluded), and scheduled to receive radiotherapy were recruited from 37 centers. Participants were randomly allocated (1:1), stratified by center and risk group, to conventionally fractionated or moderately hypofractionated radiotherapy (78 Gy in 39 fractions over 7.8 weeks or 62 Gy in 20 fractions over four weeks, respectively) or stereotactic body radiotherapy (36.25 Gy in five fractions over 1-2 weeks).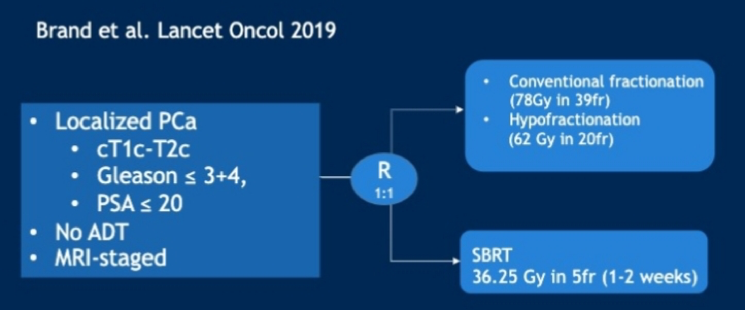
The primary endpoint of PACE-B is freedom from biochemical or clinical failure. There were 874 men to conventionally fractionated or moderately hypofractionated radiotherapy (n=441) or stereotactic body radiotherapy (n=433). Worst acute RTOG gastrointestinal toxic effect proportions were as follows: grade 2 or more severe toxic events in 53 (12%) of 432 patients in the conventionally fractionated or moderately hypofractionated radiotherapy group versus 43 (10%) of 415 patients in the stereotactic body radiotherapy group (difference -1·9 percentage points, 95% CI -6.2 to 2.4; p=0.38). Worst acute RTOG genitourinary toxicity proportions were as follows: grade 2 or worse toxicity in 118 (27%) of 432 patients in the conventionally fractionated or moderately hypofractionated radiotherapy group versus 96 (23%) of 415 patients in the stereotactic body radiotherapy group (difference -4·2 percentage points, 95% CI -10.0 to 1.7; p=0.16).
The third trial Dr. Ost discussed was the short-term androgen deprivation therapy (ADT) continued with radiotherapy as salvage treatment after radical prostatectomy for prostate cancer (GETUC-AFU 16).3 This study included patients with stage pT2, T3, or T4a (bladder neck involvement only) and pN0 or pNx according to the TNM staging system, whose prostate-specific antigen (PSA) concentration increased from 0.1 ng/mL to between 0.2 ng/mL and 2.0 ng/mL after radical prostatectomy, without evidence of clinical disease. Patients were assigned (1:1) to short-term androgen suppression (subcutaneous injection of 10.8 mg goserelin on the first day of irradiation and 3 months later) plus radiotherapy (3D conformal radiotherapy or intensity-modulated radiotherapy of 66 Gy in 33 fractions, five days a week for seven weeks) or radiotherapy alone.
Randomization was stratified according to investigational site, radiotherapy modality, and prognosis. The primary endpoint was progression-free survival (PFS) in the intention-to-treat population. There were 743 patients randomly assigned, 374 to radiotherapy alone and 369 to radiotherapy plus goserelin. At the time of data cutoff, the median follow-up was 112 months (IQR 102-123). The 120-month PFS was 64% (95% CI 58-69) for patients treated with radiotherapy plus goserelin and 49% (43-54) for patients treated with radiotherapy alone (HR 0.54, 0.43-0.68; stratified log-rank test p<0·0001).
The final study Dr. Ost discussed was the STOpCaP systematic review recently published in European Urology.4 This systematic review included trials that randomized men to prostate radiotherapy and ADT or ADT only. The review identified one ongoing (PEACE1) and two completed (HORRAD and STAMPEDE) eligible trials. Pooled results of the latter (2126 men; 90% of those eligible) showed no overall improvement in survival (HR 0.92, 95% CI 0.81-1.04, p = 0.195) or PFS (HR 0.94, 95% CI 0.84-1.05, p=0.238) with prostate radiotherapy. There was an overall improvement in biochemical progression (HR 0.74, 95% CI 0.67-0.82, p < 0.0001) and failure-free survival (FFS) (HR 0.76, 95% CI 0.69-0.84, p < 0.0001), equivalent to ∼10% benefit at three years. The effect of prostate radiotherapy varied by metastatic burden-a pattern consistent across trials and outcome measures, including survival (<5, ≥5; interaction HR 1.47, 95% CI 1.11-1.94, p=0.007). In general, there was a 7% improvement in three-year survival in men with fewer than five bone metastases.
Dr. Ost concluded with several take-away points:
- Ultrahypofractionated/SBRT is becoming a standard of care options for low- to intermediate-risk prostate cancer
- Short term ADT in addition to salvage radiotherapy improves metastasis-free survival (MFS), but not OS
- Radiotherapy to the primary improves OS for low-volume de novo metastatic prostate cancer
Written by: Zachary Klaassen, MD, MSc, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California
References:
1. Widmark, Anders, Adalsteinn Gunnlaugsson, Lars Beckman, Camilla Thellenberg-Karlsson, Morten Hoyer, Magnus Lagerlund, Jon Kindblom et al. "Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial." The Lancet 394, no. 10196 (2019): 385-395.
2. Brand, Douglas H., Alison C. Tree, Peter Ostler, Hans van der Voet, Andrew Loblaw, William Chu, Daniel Ford et al. "Intensity-modulated fractionated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): acute toxicity findings from an international, randomised, open-label, phase 3, non-inferiority trial." The Lancet Oncology 20, no. 11 (2019): 1531-1543.
3. Carrie, Christian, Nicolas Magné, Patricia Burban-Provost, Paul Sargos, Igor Latorzeff, Jean-Léon Lagrange, Stéphane Supiot et al. "Short-term androgen deprivation therapy combined with radiotherapy as salvage treatment after radical prostatectomy for prostate cancer (GETUG-AFU 16): a 112-month follow-up of a phase 3, randomised trial." The Lancet Oncology 20, no. 12 (2019): 1740-1749.
4. Burdett, Sarah, Liselotte M. Boeve, Fiona C. Ingleby, David J. Fisher, Larysa H. Rydzewska, Claire L. Vale, George van Andel et al. "Prostate radiotherapy for metastatic hormone-sensitive prostate cancer: a STOPCAP systematic review and meta-analysis." European urology 76, no. 1 (2019): 115-124.