Clinical staging of penile cancer involves palpation of the primary tumor and the inguinal nodes. However, as expected, this can often result in under-staging of the disease. Therefore, imaging modalities must be used for staging. These include MRI, CT and PET/CT.
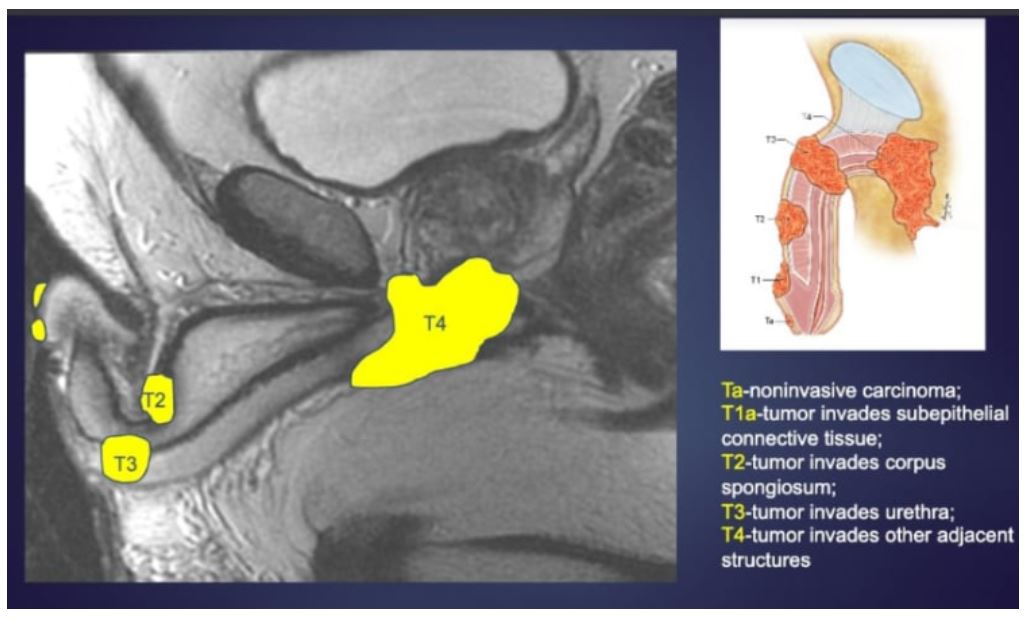
MRI can accurately predict pathological stage in 72% of cases compared to 52% using only physical examination. It can detect tunica albuginea invasion with a sensitivity of 82% and specificity of 74%, and it can detect urethral invasion with a sensitivity of 63% and specificity of 82% (Figure 1). For T staging MRI is the best modality due to its excellent soft tissue resolution.
Figure 1 – MRI for the staging of penile cancer:
Dr. Bhosale concluded her talk discussing the use of PET/CT in penile cancer. This imaging modality can be used in penile cancer, showing a sensitivity of 75% and specificity of 75% for assessment of the primary malignancy. An important tool in PET/CT is the pSUVmax which was higher in patients with tumors infiltrating subepithelial connective tissue, blood and lymphatic vessels and those with poor differentiation (pT1b and above).
PET/CT can be used for staging and to assess lymph node spread as well. Penile cancer demonstrates a predictable pattern of metastatic spread. Commonly, it spreads to the sentinel lymph node, superficial inguinal lymph nodes, inferior and deep inguinal nodes and lastly to the pelvic nodes. PET/CT should be used for staging in patients with unresectable inguinal disease, patients with comorbidities (to prevent unnecessary inguinal surgery), and for follow-up in patients who undergo chemotherapy or radiation therapy as neoadjuvant or primary therapy.
Presented by: Priya Bhosale, MD, University of Texas MD Anderson Cancer Center, Houston, Texas
Written By: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, NY, USA @GoldbergHanan at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California