A total of 886 patients were enrolled in this study with 22%, 65%, and 11% having favorable, intermediate, or poor Memorial Sloan Kettering Cancer Center (MSKCC) risk factors at baseline. Progression-free survival and objective response rate favored the combination in all MSKCC risk groups, but the median progression free survival varied, as can be seen in table 1.
Figure 1 –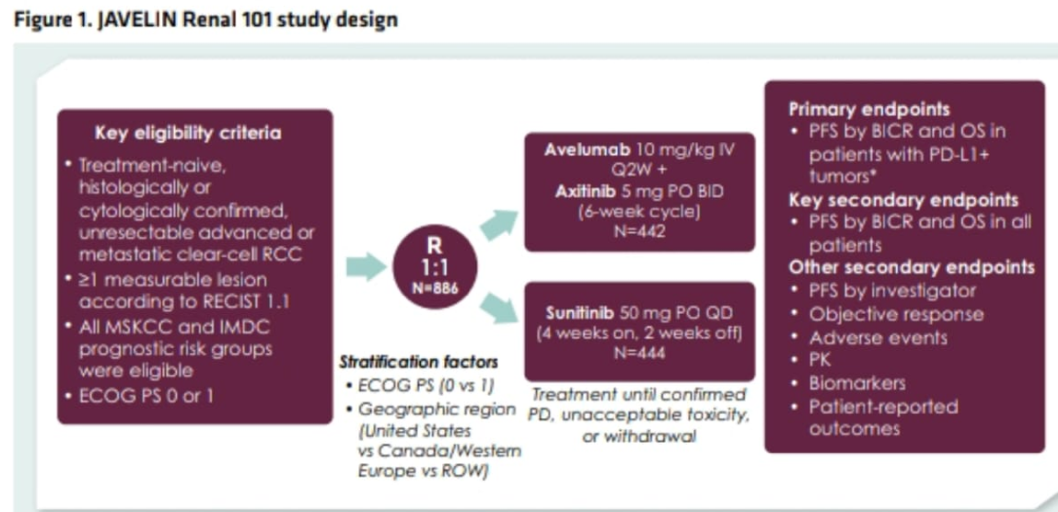
Table 1 –
The MSKCC risk groups were originally defined using empirically identified clinical characteristics. The molecular factors underlying these characteristics and their clinical significance are to date, unknown. In this presented poster, the authors report results from an analysis of baseline tumor samples from patients enrolled in the JAVELIN trial in order to define molecular characteristics underlying the MSKCC risk group classifications.
The JAVELIN renal 101 is an open label, phase 3 trial where patients were randomly assigned to receive avelumab + axitinib or sunitinib alone. The data that the authors explored are all from the post-hoc exploratory analysis based on the first interim analysis.
According to the reported results neither the presence of PD L1 immune cells nor CD8+ cells differentiated the risk groups, however, the presence of PD-L1 tumor cells was highest in the poorest risk group (p=0.0159), figure 3.

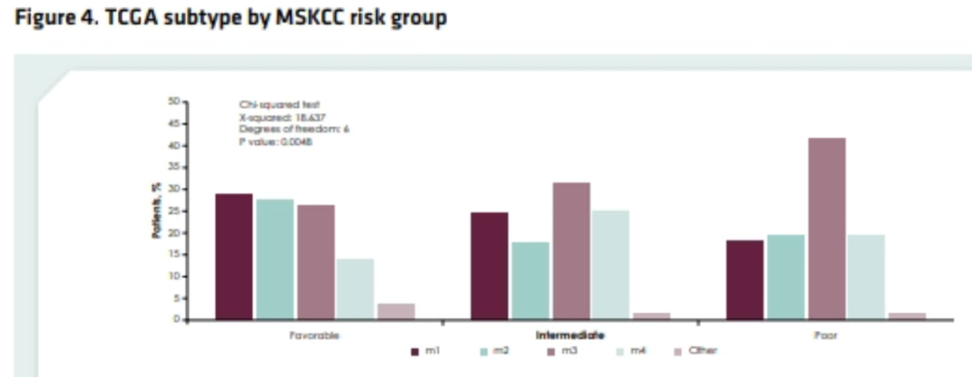
Based on the sub-type-specific mRNA signatures from the analysis of clear cell RCC by TCGA, there was a significant association between TCGA clusters and MSKCC risk groups (figure 4).
Figure 4 –
Gene expression profiling revealed differences in singular genes among the MSKCC risk groups, as shown in Table 2 and Table 3. The favorable risk group had higher expression of the organic acid metabolism and angiogenesis pathway relative to the poorest group. The favorable risk group also displayed elevated angiogenic, cytoskeleton, and lipid metabolism gene signatures, as well as reduced expression of epithelial-mesenchymal transition pathway genes.
Table 2-
Table 3-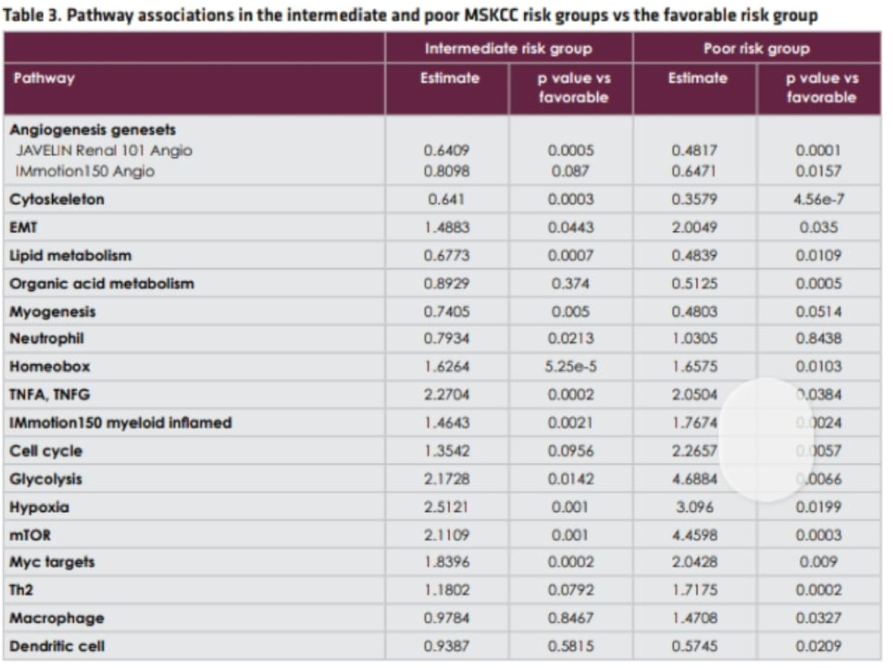
In this study of patients with advanced renal cell carcinoma, biological differences within each MSKCC risk group were shown to potentially impact response to treatment. Various molecular characteristics that differentiate the MSKCC risk groups were found. The presence of PD L1 immune cells or CD8+ cells did not differentiate between the risk groups, although the content of PD L1 was highest in the poorest risk group. Importantly, gene expression and mutations varied in the different risk groups. Although this work is promising, there is no doubt that additional analyses are needed to understand the impact of these differences in the MSKCC risk groups and their effect on responses to a standard of care RCC treatment.
Presented by: Toni Choueiri, MD, Dana-Farber Cancer Institute, Boston, MA, USA
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, NY, USA @GoldbergHanan at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California