San Francisco, California (UroToday.com) During the Oral Abstract Session C: Renal Cell Cancer at the Annual ASCO GU 2020 meeting in San Francisco, CA, Dr. Cristina Masini presented the results from phase II NIVES Study, which evaluated the efficacy and safety of SBRT in combination with nivolumab in second and third-line treatment of metastatic RCC patients. Despite the recent advances in drug therapy, patients with metastatic RCC have a 5-year survival of about 10%. Stereotactic body radiotherapy (SBRT) is a focused radiation therapy that delivers a few high doses of radiation directly to the tumor. SBRT may kill more tumor cells and cause less damage to adjacent healthy tissue. Several preclinical studies have documented an increase in peripheral anti-tumor immunity with an increased tumor antigen release, improved antigen presentation, and T-cell infiltration in the irradiated tumor. Radiation seems to synergize with immunotherapy via several mechanisms. Tumor PD-L1 expression has also been shown to be induced by radiation and inhibition of PD-1/PD-L1 axis with Nivolumab has been shown to improve anti-tumor immunity by blocking the tumor-mediated suppression of cytotoxic T cells. There are few published data of patients with solid metastatic tumors treated in clinical trials with SBRT plus immune checkpoint inhibitors (ICI). Safety, efficacy, and ideal timing of concurrent radiotherapy with ICI represents an unmet clinical need, and combining SBRT with nivolumab in patients with metastatic RCC may enhance the anti-tumor immune responses and improve the clinical outcomes.
Dr. Masini then highlighted the NIVES study design. This was a phase II, single-arm, multicenter study in metastatic RCC patients with disease progression after ≤two prior anti-angiogenic therapies with measurable metastatic sites, and at least one suitable site for SBRT. The patients received hypofractionated radiation in 1 lesion at a dose of 10 Gy/3 fractions after seven days from the first infusion of nivolumab. Nivolumab was given as a flat dose of 240 mg on day one every 14 days for six months, then 480 mg q4-weekly in responding patients until progression of the disease or unacceptable toxicity occurred. The primary endpoint was overall response rate. Secondary endpoints were progression-free survival, overall survival, overall response rate of irradiated and non-irradiated metastasis, duration of response, and safety profile. Patients were assessed for a response using RECIST 1.1 by CT every 12 weeks (+/- 1 week) until progression of disease or treatment discontinuation.
Dr. Masini then summarized the results from the NIVES study starting with patients’ baseline characteristics. Sixty-nine patients were enrolled from July 2017 to March 2019 in 12 Italian centers. 79.7% of the patients were clear cell histology, 82.6% were males, 79.7% of the patients were IMDC intermediate/poor risk category, the median age was 67 years, 18.8% of the patients were on their third line, and 21.7% of the patients did not have nephrectomy. The most frequent sites of SBRT were lung (37.7%), lymph nodes (15.9%), and bone (11.6%).
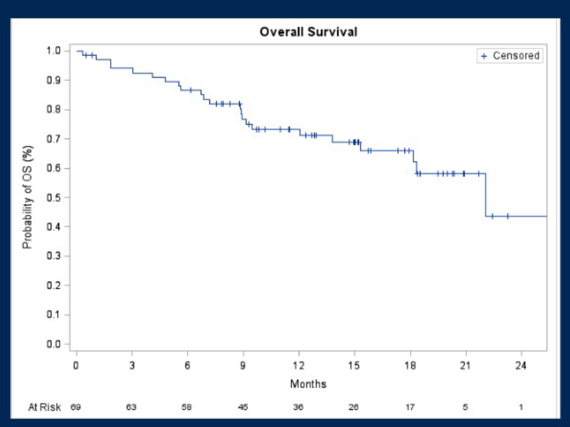
At the time of this analysis, the median number of nivolumab doses received was 12, and the median follow-up was 15 months. The overall response rate was 19%, and the disease control rate was 63.5%. The most significant benefit was noted in patients with clear cell histology. Median progression-free survival was 4.1 months, and median overall survival was 22.1 months. Twelve months progression-free survival rates were 32.6%, and overall survival rates were 73.4%. The median duration of response was 9.7 months, and the median time to response was 2.8 months. 10.1% of the patients discontinued treatment due to adverse events. Grade 3-4 toxicities related to nivolumab were experienced in 17 patients (24.6%). The most frequent Grade 3-4 toxicities included diarrhea (5.8%), an increase in amylase/lipase (4.3%), and hypothyroidism (4.3%). No Grade 3-4 toxicities related to SBRT were observed.

Dr. Masini then summarized the NIVES study with conclusions that this study represented the first prospective trial of nivolumab and SBRT combination in pre-treated mRCC patients. Nivolumab, in combination with SBRT, has an acceptable safety profile in pre-treated mRCC patients. This combination did not lead to an increase in therapy’s interruption compared to nivolumab alone. It also showed a high disease control rate and survival rate but did not reach the primary endpoints in the overall response rate. The analysis of the correlation between efficacy and PD-L1 expression/molecular alteration is ongoing in tumoral tissue samples and cfDNA. Future study directions include the different riming of SBRT and the introduction of ipilimumab and nivolumab combination.
Presented by: Cristina Masini, MD, Clinical Cancer Center, AUSL-IRCCS di Reggio Emilia, Reggio Emilia, Italy
Written by: Abhishek Srivastava, MD, Society of Urologic Oncology Fellow, Fox Chase Cancer Center, Fox Chase Cancer Center, Philadelphia, PA Twitter: @shekabhishek at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California