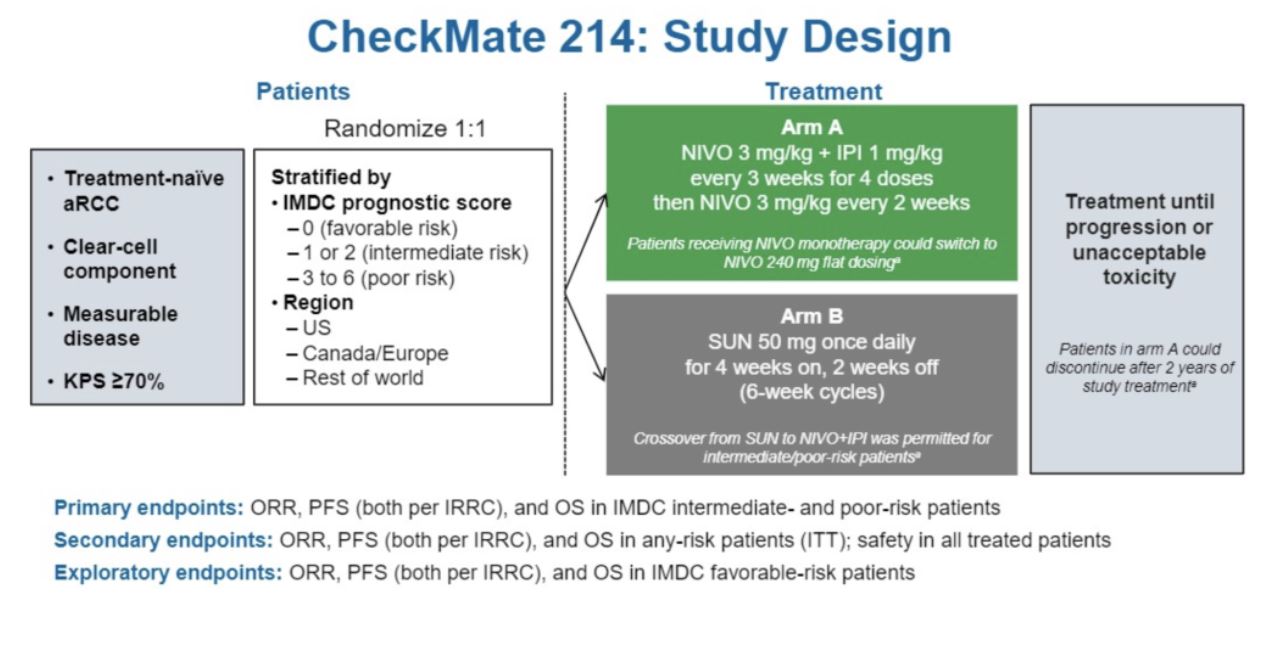
He first reviewed the study design of CheckMate-214, which is shown below with indication of the primary, secondary, and exploratory endpoints. Treatment was given until confirmed disease progression or unacceptable toxicity. Patients in each arm were balanced by IMDC risk classification (79% intermediate risk, 21% poor risk). Approximately 125 patients were included in the exploratory favorable risk study group.
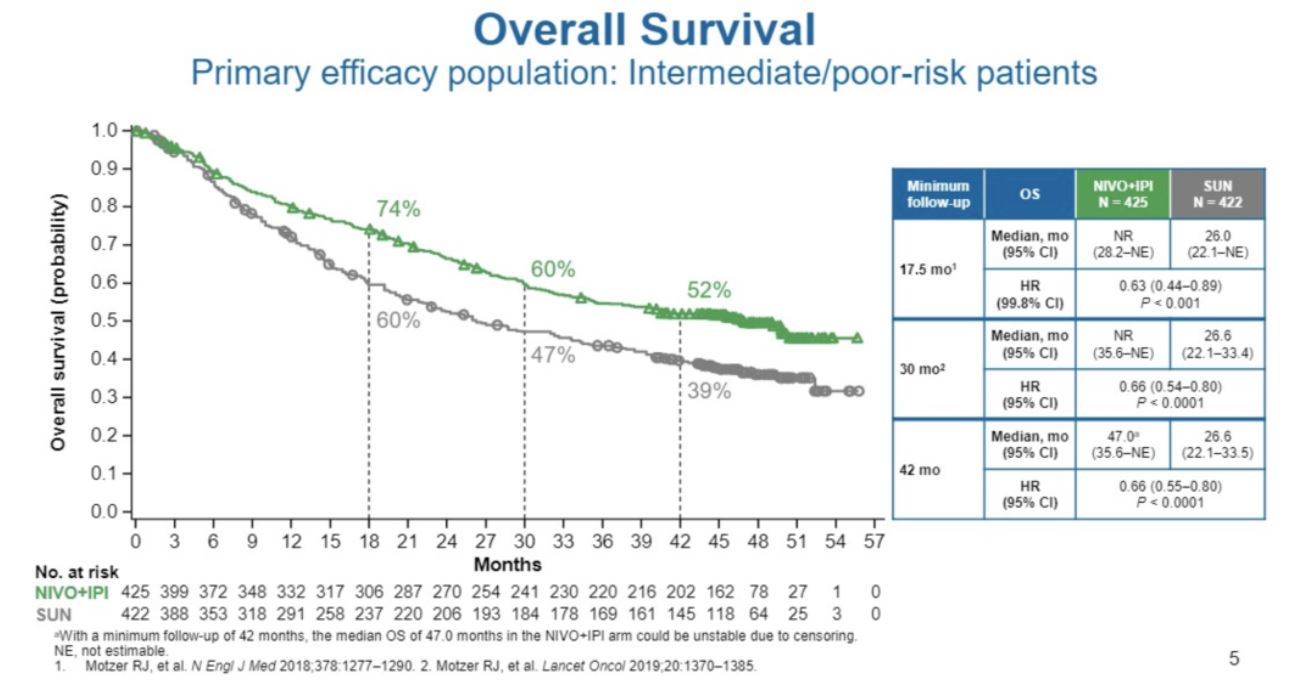
As shown in the Kaplan-Meier plot, the overall survival benefit for combination nivolumab/ipilimumab was maintained at a 42-month minimum follow-up (HR 0.66, 95% CI 0.55-0.90, P<0.0001). The median overall survival in the treatment group was 47 months versus 26.6 months in the sunitinib group.
This overall survival benefit also held true in the secondary endpoint of intention to treat analysis, though with a slightly higher hazard ratio (HR 0.72, 95% CI 0.61-0.86, P = 0.0002. The median overall survival in the sunitinib group was higher due to crossover at 38.4 months. The exploratory analysis of the efficacy of combination nivolumab/ipilimumab in favorable-risk patients compared to sunitinib showed no overall survival benefit (HR 1.19, 95% CI 0.77-1.85, P = 0.44). As expected for good risk patients, the median overall survival was not reached in either group.
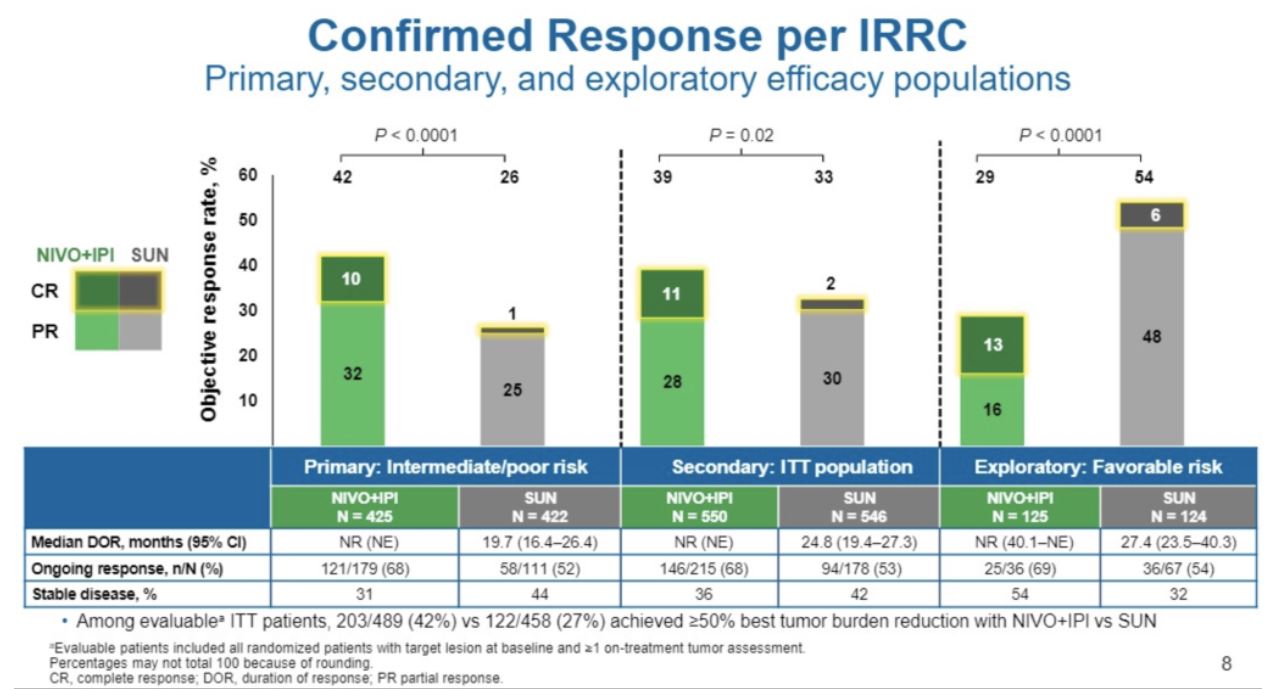
As shown below, confirmed response rates were higher with combined immune checkpoint blockade relative to sunitinib in the intermediate/poor risk group, but not in the good risk group. The median duration response of combined checkpoint blockade has not been reached.
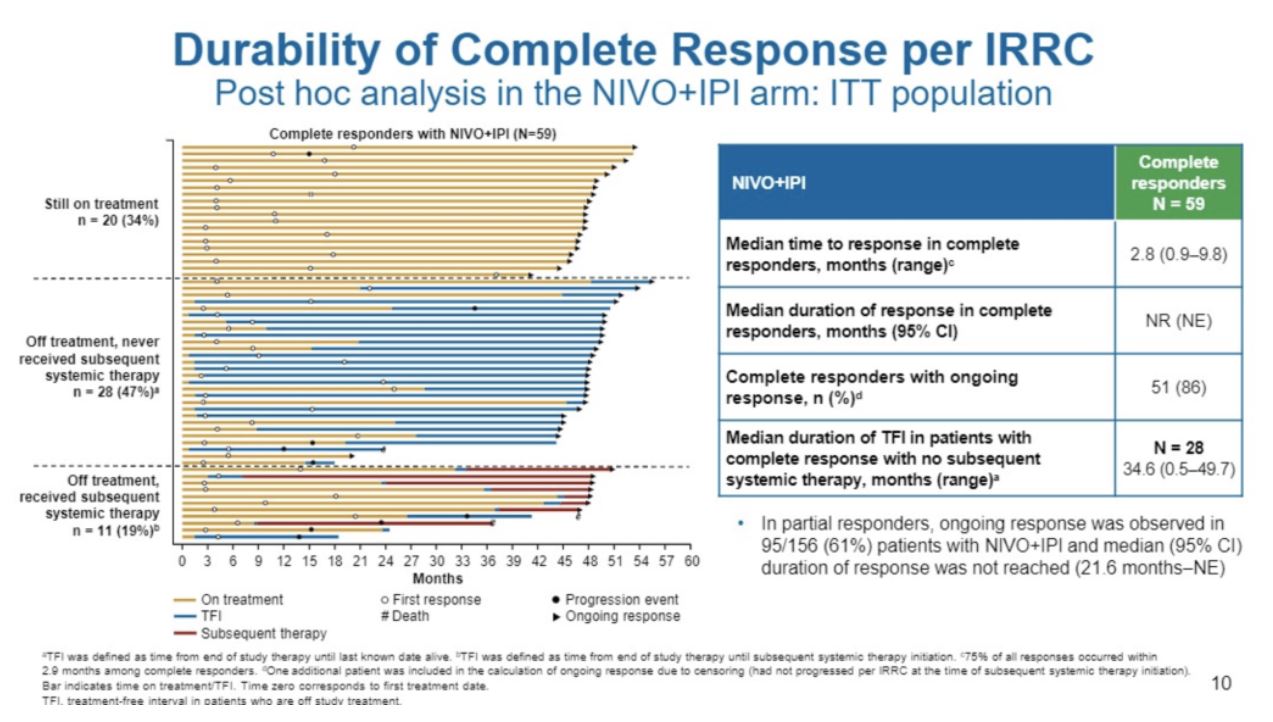
The plot below illustrates the subsequent clinical trajectory of patients that received a complete response from therapy, with 81% of patients either remaining on therapy with ongoing response or never receiving subsequent therapy to date with no disease progression. Patients with complete response were able to forgo subsequent systemic therapy for a median of 35 months.
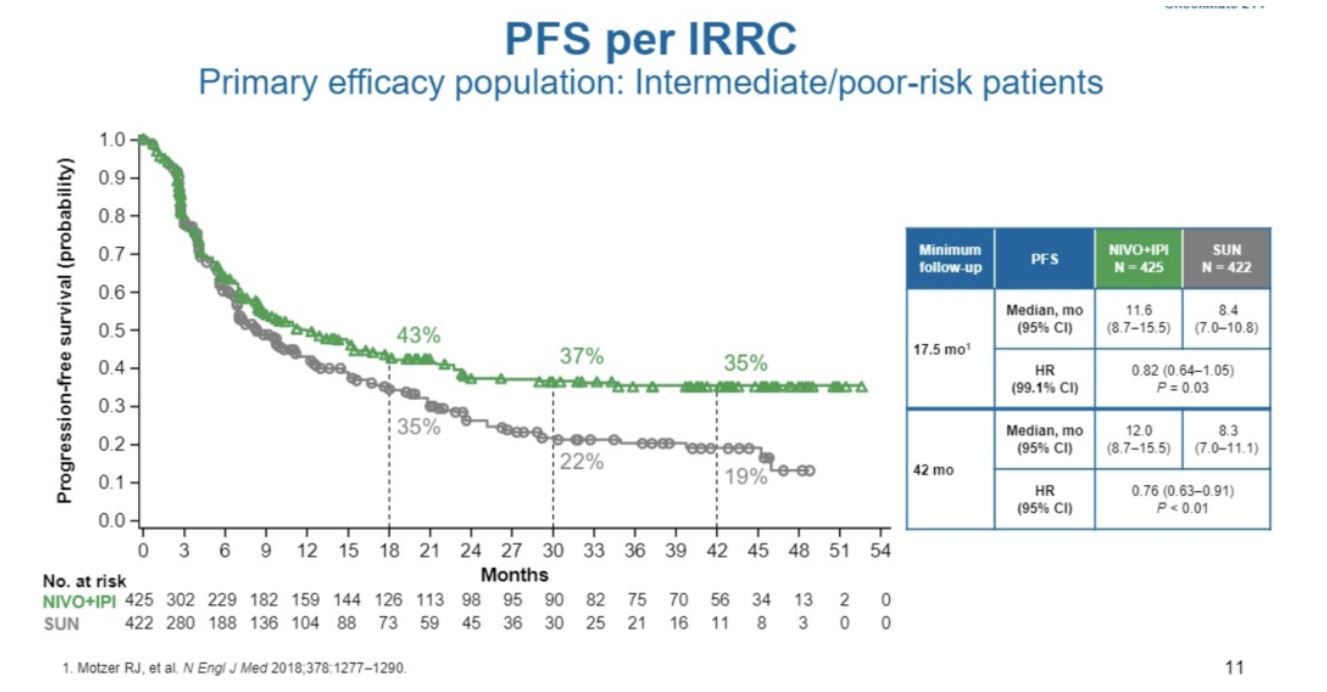
The progression-free survival Kaplan-Meier plots were also shown. Consistent with the complete response data, there was a plateau in the PFS nivo/ipi curve at 34%. There was no statistically significant PFS benefit in the intention to treat analysis, but this is outweighed by the overall survival benefit.
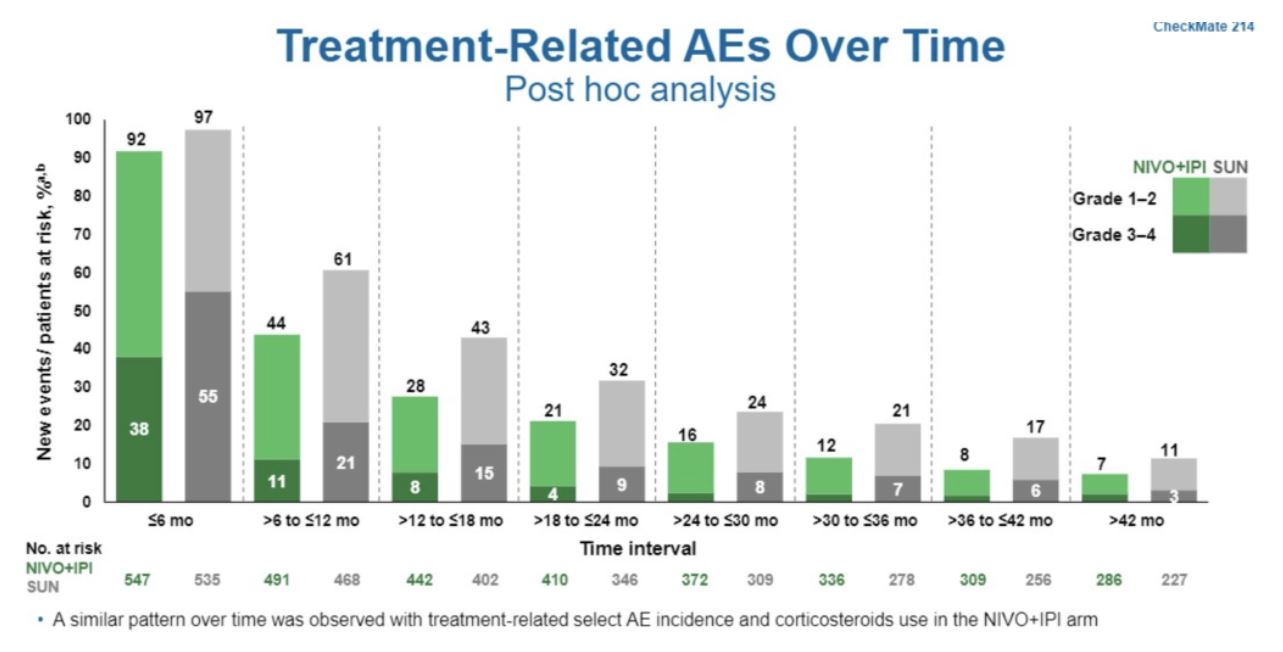
Longer-term treatment-related adverse event data was also shown. At each six month interval, the incidence of treatment-related adverse event over time was lower for combined immune checkpoint blockade compared to sunitinib, with the highest rates within the first six months
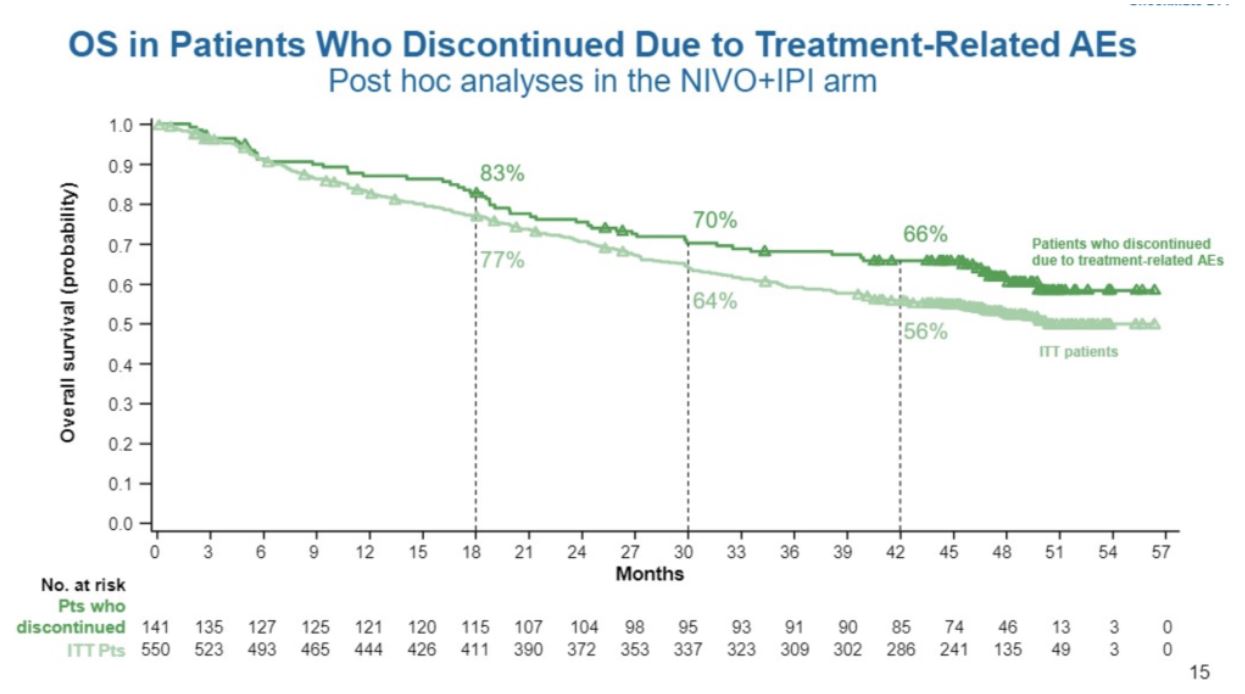
Finally, Dr. Tannir addressed the issue of survival in patients who had to discontinue immunotherapy due to adverse events. In this post-hoc analysis, overall survival probability in patients who discontinued therapy appears visually similar to the curve for patients on therapy in the intention to treat analysis.
In summary, at 42 months of minimum follow-up (median 49 months), the overall survival and objective response rate seen with combined nivolumab and ipilimumab persisted as superior to sunitinib for intermediate/poor risk patients with metastatic renal cell cancer. A significant portion of patients who experienced complete response either have been able to remain on therapy with no further disease progression or have been able to forgo any systemic therapy for years. A post hoc analysis suggests that the overall survival benefit may persist in patients despite having to discontinue therapy due to adverse side effects. No specific benefit for this combination relative to TKI therapy was seen in the good risk population, though longer follow-up will be helpful for confirming this.
Further study to understand the molecular profile of a patient who experienced a complete response and have not required further therapy will be critical for patient selection, treatment optimization, and potential treatment de-escalation.
Presented by: Nizar M. Tannir, MD, Department of Genitourinary Medical Oncology, MD Anderson Cancer Center, Houston, Texas
Written by: Alok Tewari, MD, PhD, Medical Oncology Fellow at the Dana-Farber Cancer Institute at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California