San Francisco, CA (UroToday.com) Neoadjuvant chemotherapy in resectable muscle invasive bladder cancer (MIBC) results in approximately 30% pathological complete response rates and is associated with improved patient survival. In this presentation, Dr. Syed Hussain presented results from the NEO-BLADE study, which adds the tyrosine kinase inhibitor nintedanib (antagonizes PDGFR, FGFR-1, VEGFR-2) to standard of care gemcitabine and cisplatin. Prior trials with other TKIs such as sunitinib have been hampered by toxicity issues.
In this phase 2 trial of nintedanib or placebo in combination with standard of care chemotherapy, 120 patients were enrolled in order to detect an improvement of 20% in the primary endpoint of pathological complete response (pCR). The co-primary endpoint was overall CR rate as measured by either pCR or radiological CR. The secondary endpoints were progression free survival, overall survival and toxicity. Patients were eligible for enrollment if they were found to have cT2-T4N0M0 transitional cell carcinoma and GFR > 60. The study schema is shown below. Interestingly, this trial allowed for either cystectomy or organ preservation surgery. pCR was therefore either identified by cystectomy sampling or post-treatment biopsy.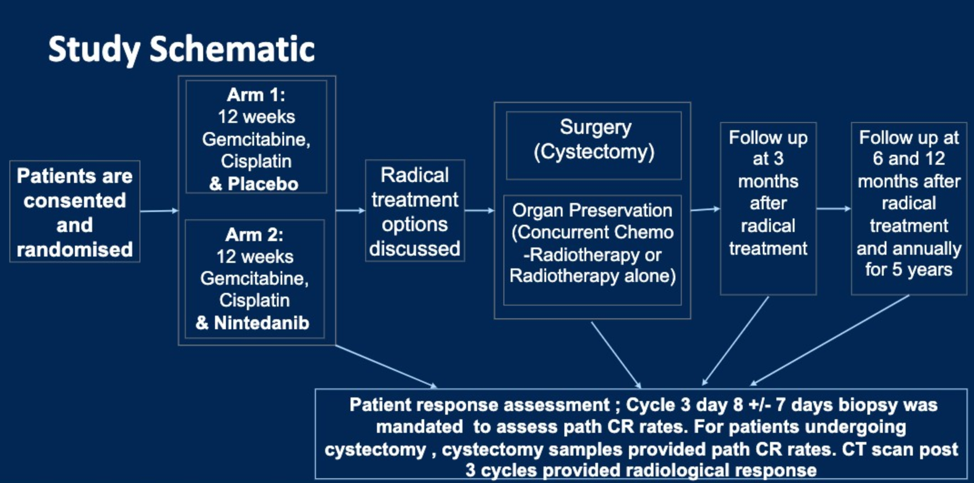
The clinical characteristics of patients enrolled on the trial are shown below. Gemcitabine was given at 1000 mg/m2 on days 1 and 8, and cisplatin was given at 70 mg/m2 on day 1 but dose splitting was allowed for GFR < 60. Nintedanib was given at 200 mg BID. Based on a lead-in safety study, patients whose GFR dropped to < 60 were given 35 mg/m2 cisplatin and 1000 mg/m2 gemcitabine on days 1 and 8 along with 150 mg Nintedanib BID.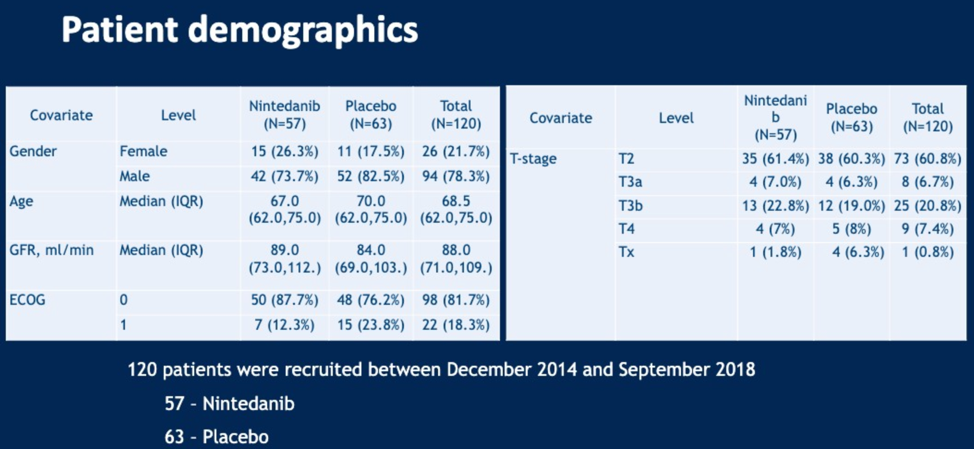
There was no statistically significant difference in the primary endpoints of pCR (OR 1.31, 95% CI 0.84-2.06) or overall CR rate (OR 0.90, 95% CI 0.60-1.35). There was a statistically significant difference, however, in the secondary endpoints of progression free survival and overall survival between the arms. The median PFS in the standard of care group was 16.7 months, and the median PFS in the nintedanib group was not reached. Therefore, the addition of nintedanib conferred a hazard ratio against disease progression of 0.468 (95% CI 0.254-0.863, P = 0.013). The median overall survival in the standard of care group was 50.6 months and this was not reached in the nintedanib arm. The hazard ratio for death was therefore 0.379 with the addition of nintedanib (95% CI 0.165-0.874, p=0.018).
With regards to safety, the addition of nintedanib resulted in increased rates of neutropenia and hypertension, but otherwise did not significantly alter the toxicity profile of standard of care gemcitabine and cisplatin.
Tissue, blood, and urine are available for molecular correlates of clinical benefit. The mechanism of improved survival may be related to nintedanib effect on the tumor microenvironment via FGFR inhibition, but more extensive molecular studies are required.
Though not associated with improved rates of pCR or overall CR, the PFS and OS benefit of adding nintedanib from this phase 2 trial are compelling and will likely be further evaluated in a phase 3 clinical trial.
Presented by: Syed A. Hussain, MD, University of Sheffield, Academic Unit of Oncology, Department of Oncology and Metabolism, Sheffield, United Kingdom
Written by: Alok Tewari, MD, PhD, Medical Oncology Fellow at the Dana-Farber Cancer Institute, at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California