This study examined whether or not a CTC change, PSA50, or the combination of the two variables could be used as a surrogate endpoint for overall survival in clinical trials. This study used the CellSearch® (Menarini) platform to count CTCs.

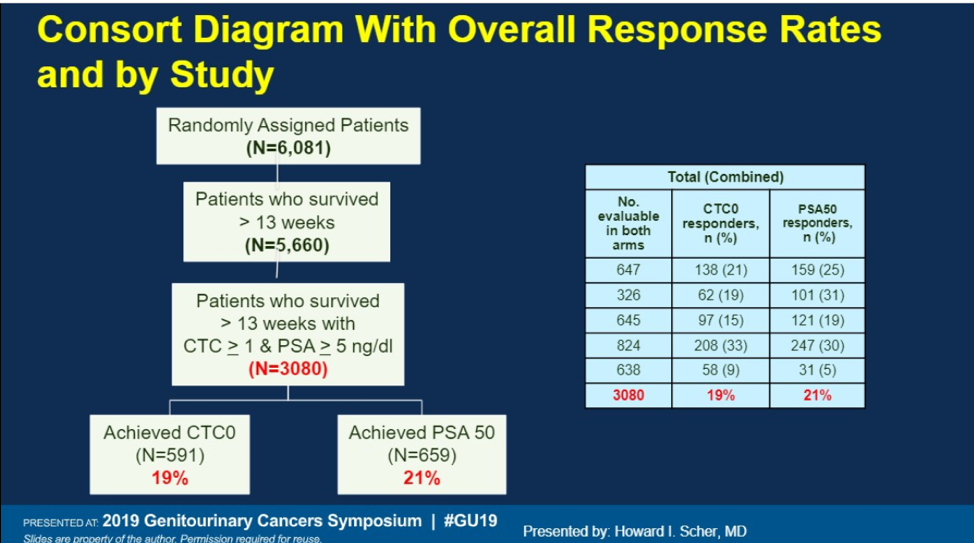
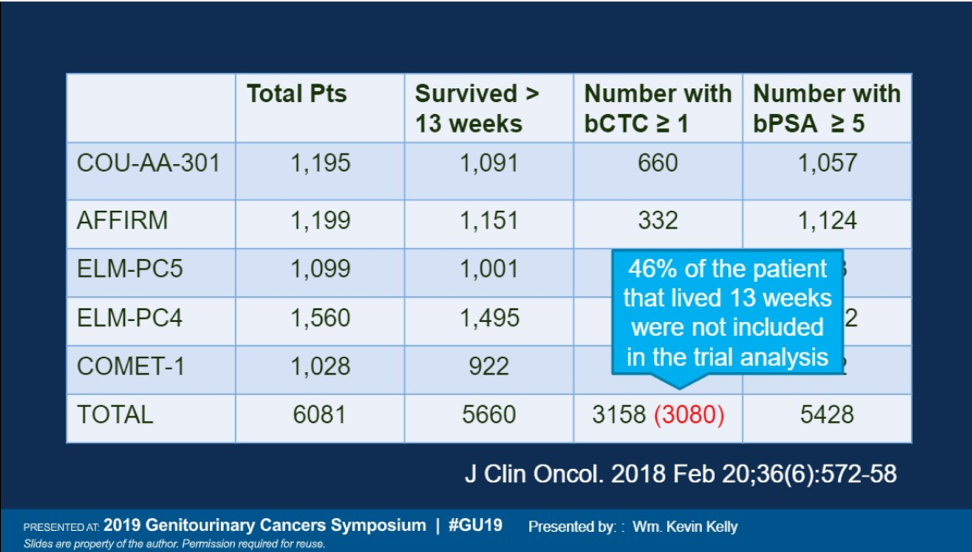
Data from 5 randomized mCRPC trials were included (shown above). PSA and CTC counts were collected at baseline and at 13 weeks, and overall survival was analyzed with respect to four variables: PSA50 (≥ 50% PSA decline from baseline), CTC0 (≥ 1 CTC/7.5 ml of blood at baseline and 0 CTCs at week 13), both PSA50 and CTC0, and either PSA50 or CTC0. A total of 6081 patients were analyzed from 5 clinical trials, of which 93% were alive at 13 weeks for measurement of CTCs and PSA. 3080 (54%) of patients had detectable CTCs at baseline.
In terms of overall survival analysis, change in CTCs from detectable to undetectable provided the greatest separation between responders and non-responders, more than PSA50 or the combination CTC change and PSA50.
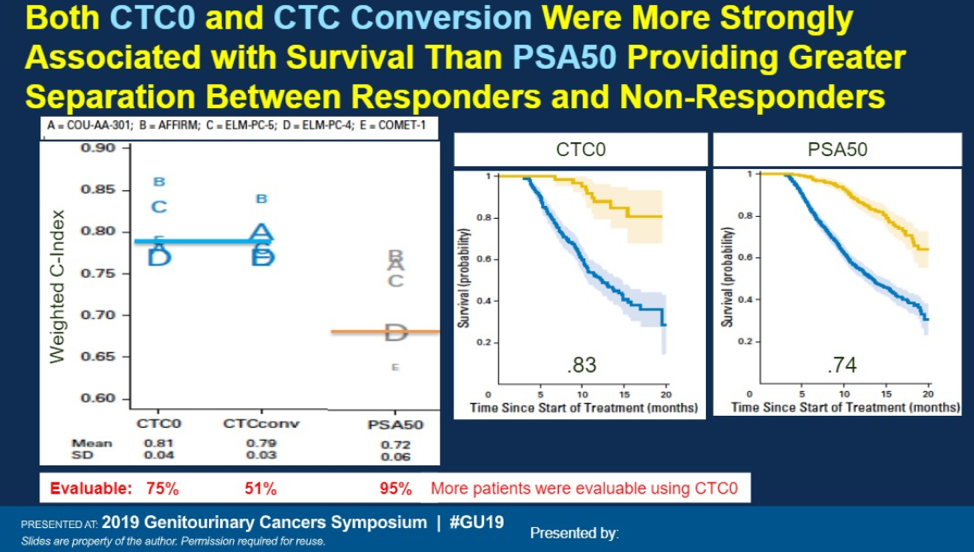
CTC change from detectable to undetectable at week 13 may provide an early signal of benefit for patients with mCRPC and may actually provide a stronger measure of response compared with PSA50. However, there are significant limitations of this strategy. A significant number of patients do not have a detectable baseline CTC count and therefore may not be assessable using a CTC response measure. In the AFFIRM trial, 63% of patients did not have a baseline CTC. In this study, 46% of patients were not included due to CTC criteria.
Also, regardless of the biomarker, 14-18% of patients do not survive to 13 weeks, and this may bias any study that requires a week 13 biomarker. Additional prospective studies are necessary to see if CTC0 is predictive of overall survival in other disease states as well as with non-AR directed therapies.
Presented by: Howard I. Scher, MD, FASCO, Medical Oncologist, Co-Chair, Center for Mechanism Based Therapy; Head of the Biomarker Development Initiative; D. Wayne Calloway Chair in Urologic Oncology, Memorial Sloan Kettering Cancer Center
Discussant: William Kevin Kelly, DO
Written by: Jason Zhu, MD. Fellow, Division of Hematology and Oncology, Duke University, Twitter: @TheRealJasonZhu at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA
References:
- Alix-Panabières C, Pantel K. Clinical applications of circulating tumor cells and circulating tumor DNA as liquid biopsy. Cancer discovery 2016;6:479-91.
- Scher HI, Heller G, Molina A, et al. Circulating tumor cell biomarker panel as an individual-level surrogate for survival in metastatic castration-resistant prostate cancer. Journal of clinical oncology 2015;33:1348.
- Lorente D, Olmos D, Mateo J, et al. Circulating Tumor Cell Increase as a Biomarker of Disease Progression in Metastatic Castration-Resistant Prostate Cancer Patients with Low Baseline CTC Counts. Annals of Oncology 2018.
- Heller G, McCormack R, Kheoh T, et al. Circulating tumor cell number as a response measure of prolonged survival for metastatic castration-resistant prostate cancer: A comparison with prostate-specific antigen across five randomized phase III clinical trials. Journal of Clinical Oncology 2018;36:572.