In patients with castration resistant prostate cancer and bone metastasis, a randomized, placebo-controlled trial in 2002 showed that zoledronic acid significantly reduced skeletal related events compared to those who received placebo and increased the median time to first skeletal related event1. Denosumab, a humanized monoclonal antibody which binds to RANK ligand, has also been shown to significantly delay the first skeletal related event, even more so than zoledronic acid in a randomized double blind study2. In a phase III study with 1904 patients (950 assigned to denosumab and 951 assigned to zoledronic acid), median time to first on-study skeletal-related event was 20.7 with denosumab compared with 17.1 months with zoledronic acid (hazard ratio 0.82, 95% CI 0.71-0.95; pp = 0.008). In that study, denosumab and zoledronic acid were given every four weeks. However, the optimal schedule of denosumab is unknown, and there does appear to be a dose dependent increase in osteonecrosis of the jaw3.
Summary
In this open label, randomized phase III non-inferiority study, the authors sought to determine what the time to first on trial symptomatic skeletal event was, defined as clinically significant pathologic fracture, radiation therapy to bone, or surgery to bone or spinal cord compression. The investigators also measured safety, time to first and subsequent on trial SSE, skeletal morbidity rate, quality of life, and health economic outcomes. The main hypothesis to be tested was whether or not denosumab efficacy is maintained at every 12 weeks compared with every 4 weeks.

Eligibility criteria included patients with CRPC who had 3 more or bone metastases, a performance status of 0-2, corrected calcium of ≥2 mmol/L and ≤3 mmol/L with no history of osteonecrosis.
690 patients were randomly assigned to every 4 weeks vs every 12 weeks after a induction phase which included four doses given every 4 weeks. This interim analysis was completed after 3.5 years of trial accrual and all patients on study were placed on supplementation of calcium and vitamin D. Data from 282 patients is represented here.
During every four week induction phase, 28.7% of men experienced hypocalcemia. However, for patients who were switched to the every 12 week regimen, 52.3% of patients had improvement in hypocalcemia grade, compared with 26.3% of patients who rained on the every 4 week schedule.


The incidence of all grade hypocalcemia was 40.2% for patients on q4 week treatment compared to 20.3% on q12 weekly treatment.
The rate of hypocalcemia shown in this trial was significantly higher than the initial denosumab vs zoledronic acid trial.

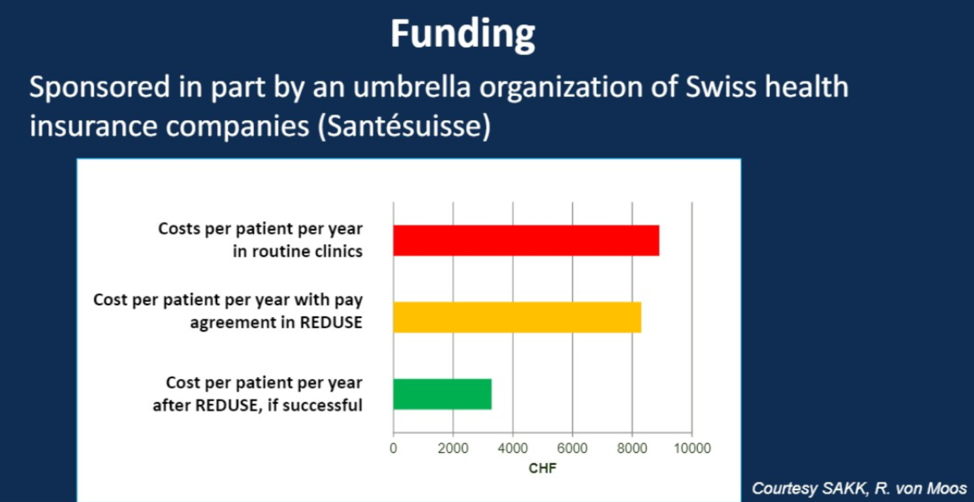
Lastly, and importantly, the author noted that this study was funded by an umbrella organization of Swiss health insurance companies and that this may be a promising source of funding for future drug de-escalation studies.
Conclusions
More patients (39%) experienced hypocalcemia than was previously reported in registration trials of denosumab (13%). The primary endpoint of this study has not been reported yet and Dr. Gillessen did not recommend making q12 week denosumab standard of care yet during the Q&A session. Clinicians should always be mindful of patients’ vitamin D and calcium levels prior to treatments with denosumab and continue supplementation throughout treatment. Future drug de-escalation studies may be successfully funded by insurance companies.
Presented by: Silke Gillessen, MD, Professor and Chair in Genitourinary Oncology Systemic Therapy Research at The University of Manchester and The Christie NHS Foundation Trust, Co-founder of the Advanced Prostate Cancer Consensus Conference (APCCC
Written By: Jason Zhu, MD. Fellow, Division of Hematology and Oncology, Duke University, Twitter: @TheRealJasonZhu at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA
References:
1. Saad F, Gleason DM, Murray R, et al. A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. Journal of the National Cancer Institute 2002;94:1458-68.
2. Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. The Lancet 2011;377:813-22.
3. Kyrgidis A, Toulis K. Denosumab-related osteonecrosis of the jaws. Osteoporosis international 2011;22:369-70.