Squamous cell carcinoma of the penis, or penile cancer, has an established drainage pathway through the superficial inguinal nodes, deep inguinal nodes and then to the pelvic lymph nodes. To reflect this, the staging for penile cancer has stratified nodal staging into 4 substages – pN0 – N3, based on the presence of lymph nodes, number of lymph nodes, laterality, and mobility. However, lymph node involvement isn’t clear cut! He points out that while 25% of cN0 patients harbor micrometastatic disease, up to 50% of patients with cN1/2 disease are pN0 (due to inflammatory and reactive lymph nodes). This makes management slightly more nuanced.
Historically, inguinal lymph node dissection (ILND) has represented the most effective treatment for PeCa nodal metastases – and provided the only real opportunity for cure. As has been evidenced numerous times, nodal involvement is the strongest prognostic indicator of survival in PeCa – and patients with low-volume mets with node dissection have a potential for durable response and cure. He cited the Djajadiningrat et al. (J Urol 2014) paper, which identified that cancer-specific mortality was associated strongly with cN and pN status.
The usual approach to nodal management is to complete an ILND in patients with high-risk disease – and patients with deep inguinal lymph node involvement should warrant PLND as well. Dr. Nicolai’s group looked at predictors of having pelvic lymph node disease (Lughezzani G et al.) – and in their work, PLND can be safely spared in men with the following features: no extranodal extension, < 3 lymph nodes involved, and < 3 cm in tumor size. All other patients warranted PLND, as even one of these features resulted in >10% involvement of ipsilateral lymph nodes.
In his mind, patients with nodal metastases can be grouped into 2 risk categories:
- Early, favorable N+ (patients who were cN0-1 and ended up pN1-2) – and in these patients, surgery can have durable survival (60+% in some series)
- Bulky N+ disease (cN3 or pN3) – these patients have durable remissions <30%.
- Chemotherapy
- Which regimen?
- Neoadjuvant or adjuvant?
- Radiation therapy
- Alone or with chemo?
- Can it be given with chemo, but without surgery?
He noted 4 adjuvant chemotherapy studies – some of which are very old and utilize toxic chemotherapy regimens (PVB). The most recent series is by his group (Nicolai N et al. Clin Gen Cancer 2016), which utilized T-PF in 19 patients with pN2-3 disease and found a 52% response rate. The 4 studies are summarized below:

Sharma P et al. (Urol Onc 2015) found in a multi-institutional retrospective series (which all the limitations and biases that go with it) that AC was associated with improved OS.
Neoadjuvant chemotherapy:
There is more data in the neoadjuvant setting. Major studies are summarized below:
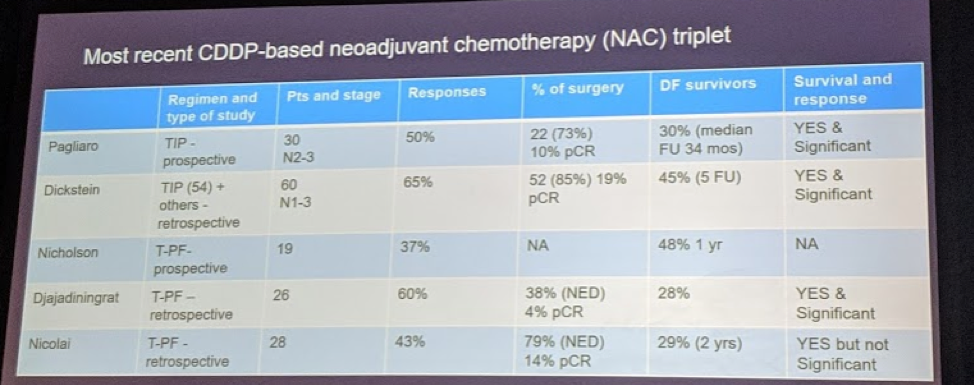
Response rates ranged from 35-60% with improved survival – primarily in patients with N2-3 disease. TIP and T-PF were th primary regimens utilized.
Current guidelines recommend NAC for patients with bulky palpable or fixed unilateral or bilateral nodes. AC is recommended for patients >= 2 positive inguinal nodes or extranodal extension on final pathology.
Lastly, in a paper by Necchi et al. (Clin Gen Cancer 2017), the authors compared AC and NAC in a retrospective institutional series – and again, with the inherent biases of retrospective study and immortal time bias of AC studies, they found that AC was associated with significantly improved recurrence-free survival (RFS) but not OS.
Ultimately, for patients with bulky nodal disease, AC or NAC is recommended, but uncertain which one is better. He does note that due to the morbidity of the ILND, many patients who deserve systemic therapy may never get AC – so, it may be better to get NAC and increase exposure.
Radiation therapy:
He didn’t touch much on the role of radiation and deferred to Dr. Hoffmann’s talk. Yet, he did again state that there is insufficient data at this time.
Inguinal LND Morbidity:
He notes that ILND is a highly morbid procedure, with high rates of skin necrosis, lymphedema, infection, seroma, and lymphocele. He briefly touched upon techniques to help reduce the morbidity, including limited ILND (in cN0 patients), dynamic sentinel lymph node biopsy (in cN0 patients), and robotic/laparoscopic ILND (associated with reduced skin related complications, but no difference in lymphedema/lymphoceles).
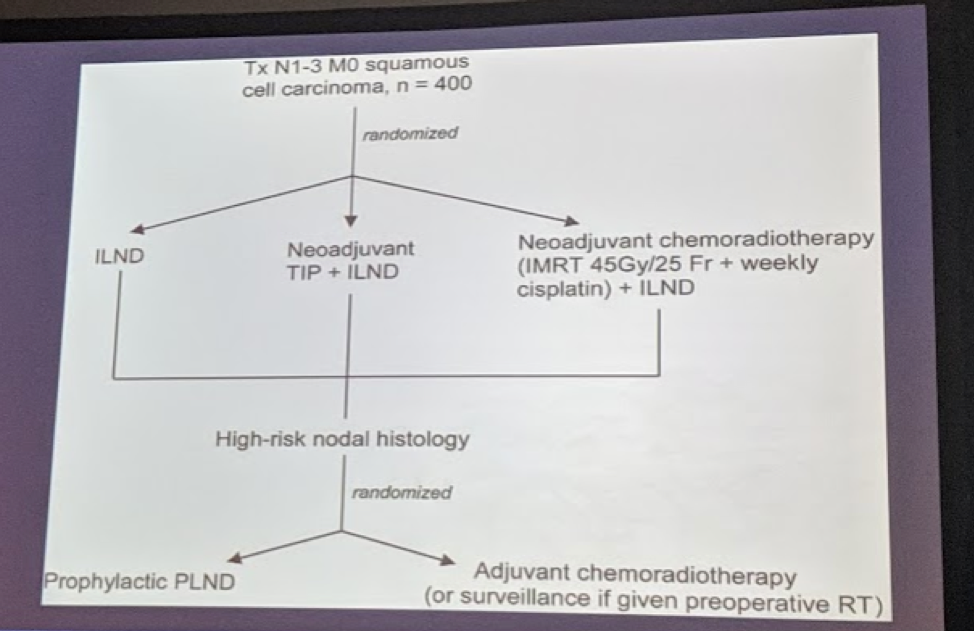
InPACT study
Lastly, he touched upon the InPACT study, as Dr. Hoffmann did. In this study, node-positive patients are randomized to ILND, NAC + ILND, and neoadjuvant chemoradiation + ILND. Following ILND, patients were then randomized to prophylactic PLND or adjuvant chemoradiation therapy.
Written by: Thenappan Chandrasekar, MD (Clinical Instructor, Thomas Jefferson University) (twitter: @tchandra_uromd, @JEFFUrology) at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA