
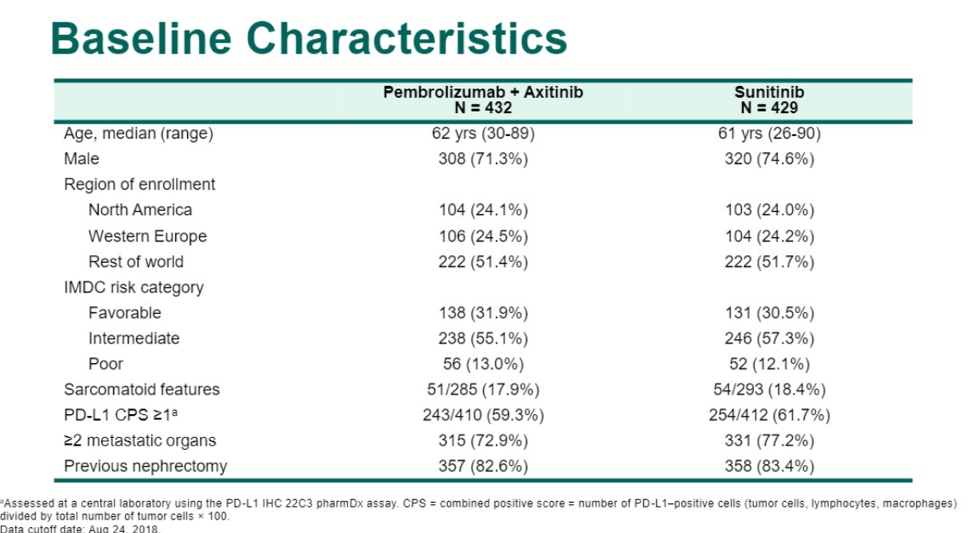
A total of 861 patients were enrolled in the study. The median age was 62 in the pembrolizumab arm and 61 in the sunitinib arm. The majority of patients were men (71%) and had intermediate or poor risk disease by IMDC criteria. This cohort also contained a high percentage of patients who were deemed PD-L1 positive, based on a CPS ≥1 (roughly 60% in both arms). Also, unlike many patients in the post-CARMENA era, the majority of patients had a previous nephrectomy (82%).

Presented by: Thomas Powles, MD, PhD, FCRP, Professor of Genitourinary Oncology, Lead for Solid Tumour Research at Barts Cancer Institute, Director of Barts Cancer Centre
Written by: Jason Zhu, MD. Fellow, Division of Hematology and Oncology, Duke University, @TheRealJasonZhu at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA
References:
- Lee C-H, Makker V, Rasco DW, et al. Lenvatinib+ pembrolizumab in patients with renal cell carcinoma: Updated results. American Society of Clinical Oncology; 2018.
- Choueiri TK, Larkin JMG, Oya M, et al. First-line avelumab + axitinib therapy in patients (pts) with advanced renal cell carcinoma (aRCC): Results from a phase Ib trial. Journal of Clinical Oncology 2017;35:4504-.
- Atkins MB, Plimack ER, Puzanov I, et al. Safety and efficacy of axitinib (axi) in combination with pembrolizumab (pembro) in patients (pts) with advanced renal cell cancer (aRCC). Journal of Clinical Oncology 2018;36:579-.
- Escudier B. Combination Therapy as First-Line Treatment in Metastatic Renal-Cell Carcinoma.0:null.