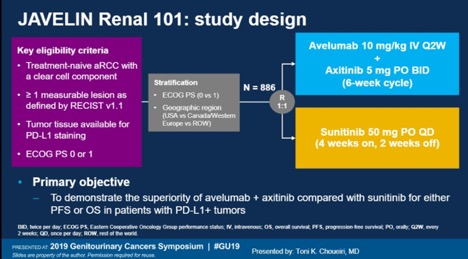
JAVELIN 3 is an going phase III study which evaluates avelumab + axitinib (AA) versus sunitinib for patients with previously untreated advanced renal cell carcinoma. Avelumab was given 10 mg/kg every 2 weeks and axitinib was given 5 mg twice daily. Sunitinib 50 mg was given on a 4 week on, 2 week off schedule. At the time of data cutoff in June 2018, the median follow up time was 12 months for the AA arm and 11.5 months for the sunitinib arm.
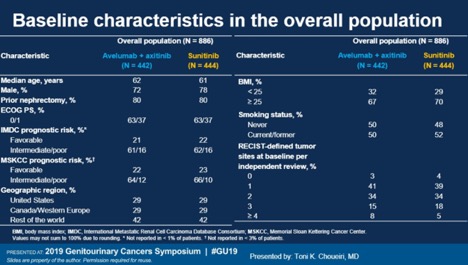
A total of 886 patients were randomized to AA or sunitinib. The baseline characteristics were well balanced. Patients were balanced by age, prior nephrectomy (80% in both arms), IMDC risk (~80% were poor/intermediate risk), and geographic region. Due to some data which had correlated BMI and smoking status with outcomes in RCC, patients were also balanced for BMI (~70% had a BMI≥25) and 50% were never smokers3,4.
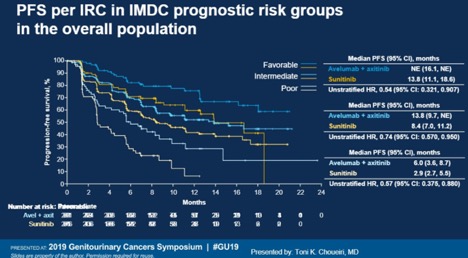
In terms of PFS per IMDBC risk groups, AA outperformed sunitinib for every risk group. For patients with MSKCC favorable risk disease, the median PFS has not yet been reached and was 13.8 months in the sunitinib arm (HR 0.54). For intermediate risk patients, mPFS was 13.8 months vs 8.4 months favoring AA, and for poor risk patients, mPFS was 6.0 vs 2.9 months also favoring AA.
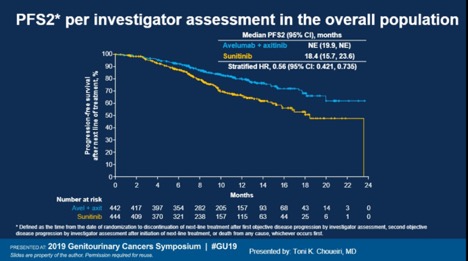
Median PFS2, defined as the time from date of randomization to discontinuation of the next line of therapy, was not yet reached for AA and was 18.4 months for sunitinib. For patients who progressed on the sunitinib arm, 67% of patients were subsequently treated with a checkpoint inhibitor.
Objective response rate was 66% for favorable risk, 50% for intermediate risk, and 31% of poor risk. PD-L1 status did not consistently discriminate between responders and non-responders. Patients defined as PD-L1+ had an ORR of 55% compared to 47% of PD-L1 negative.
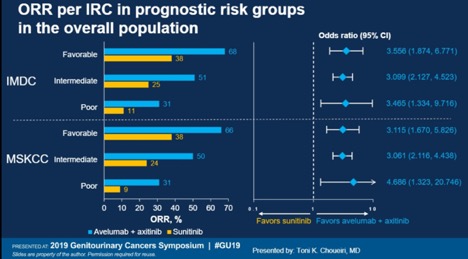
Avelumab plus axitinib joins the list of combination therapies which appear very promising for the front-line treatment of mRCC. Unlike combination ipilimumab/nivolumab which did not demonstrate benefit for patients with good risk disease, this is the space where AA thrives, with a 66% response rate.
An excellent comparison by Dr. Escudier compares the this trial to the Pembrolizumab+axitinib study5. The study populations are fairly similar in terms of IMDC risk populations as well as patients with the percentage of patients with quantifiable PD-L1 expression ≥1%. However, at this time, pembrolizumab + axitinib has an OS benefit over sunitinib whereas this endpoint has not yet been reached for AA+sunitinib. However, this may change with longer follow up and future results may show an OS benefit for this combination, given the durability of responses of patients on immune checkpoint inhibitors as we have seen in numerous other trials.
Presented by: Toni K. Choueiri, MD, Dana Farber Cancer Institute, Boston, Massachusetts
Written by: Jason Zhu,MD, Fellow, Division of Hematology and Oncology, Duke University. Twitter: @TheRealJasonZhu at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA
References:
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. New England Journal of Medicine 2018;378:1277-90.
- Choueiri TK, Larkin JM, Oya M, et al. First-line avelumab+ axitinib therapy in patients (pts) with advanced renal cell carcinoma (aRCC): Results from a phase Ib trial. American Society of Clinical Oncology; 2017.
- Waalkes S, Merseburger AS, Kramer MW, et al. Obesity is associated with improved survival in patients with organ-confined clear-cell kidney cancer. 2010;21:1905-10.
- Kroeger N, Klatte T, Birkhäuser FD, et al. Smoking negatively impacts renal cell carcinoma overall and cancer‐specific survival. 2012;118:1795-802.
- Escudier B. Combination Therapy as First-Line Treatment in Metastatic Renal-Cell Carcinoma N Engl J Med. 2019 Feb 16. doi: 10.1056/NEJMe1900887