Dr. Efstathiou started by noting that there has been a paradigm shift in contemporary oncology in that organ conservation is commonplace – this is specifically true for laryngeal carcinoma, anal carcinoma, breast carcinoma, esophageal carcinoma, and limb sarcomas. He states that a radical cystectomy is life-altering and has significant morbidity. In a study of 1,142 radical cystectomies performed at Memorial Sloan Kettering Cancer Center, more than 64% of patients had more than one complication, 13% had a grade 3-5 complication, 26% of patients were readmitted and the 90-day mortality rate was 2.7% [1]. Dr. Efstathiou questions how golden it the “gold standard” radical cystectomy? He highlights that the recurrence rates in the pelvis are not low (41%) and late complications are not low. At 10 years after radical cystectomy, >70% have renal deterioration, >50% have new onset CKD stage 3 and 3.5% will progress to hemodialysis.
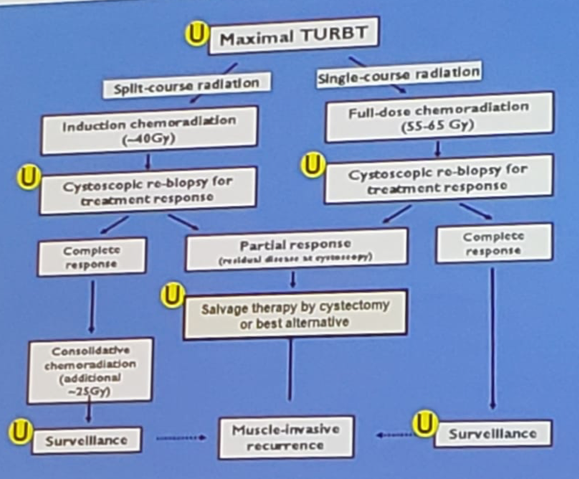
Dr. Efstathiou mentioned that radical cystectomies are not being performed in ~50% of patients, and as such, there is a huge unmet need, of which TMT can fill that gap. This is particularly evident in patients >70 years of age. For the surgeons who think TMT may take away the surgical aspect of MIBC, Dr. Efstathiou notes that TMT is very much a surgical approach – in his mind, urologists are the quarterback for TMT as noted in the following algorithm (U denotes urologist):
To support this, he notes that a quality/aggressive TURBT and salvage cystectomy (for the 10-15% that require it) is paramount to the success of TMT2. At Massachusetts General Hospital, Dr. Efstathiou says that they have excellent long-term results with TMT that are comparable to radical cystectomy: among cT2 disease, 5-year DSS is 74% and 10-year DSS is 66%2. Among patients treated in a contemporary setting (2005-2013), salvage cystectomy rates are only 15%2. Dr. Efstathiou cautions that population-level database studies should be interpreted with extreme care, secondary to (i) patients unfit for surgery are not excluded, (ii) median radiotherapy fraction was 18 (typically >30 are needed for definitive therapy), (iii) confounding, misclassification, and selection bias is high.
According to Dr. Efstathiou, the most important study and compelling argument for TMT is from a propensity score-matched analysis from Toronto by Kulkarni et al.3 Data from patients treated in a multidisciplinary bladder cancer clinic from 2008 to 2013 were reviewed and those who received TMT for MIBC were identified and matched with propensity scores to patients who underwent radical cystectomy. A total of 112 patients with MIBC were included after matching (56 in each group), and at a median follow-up of 4.5 years, there were 20 deaths (35.7%) in the radical cystectomy group (13 as a result of bladder cancer) and 22 deaths (39.3%) in the TMT group (13 as a result of bladder cancer). The 5-year DSS rate was 73.2% and 76.6% in the radical cystectomy group and TMT groups, respectively (p = 0.49).
Concurrent chemotherapy is important to the success of TMT, and Dr. Efstathiou notes that there are several active radiosensitizing drugs, including cisplatin, paclitaxel, 5-FU, mitomycin C, low-dose gemcitabine, and carbogen/nicotinamide. Furthermore, long-term toxicity is acceptable and quality of life after bladder preservation is good and likely better than radical cystectomy. This includes better sexual QoL, fewer concerns about appearance, and less interference from cancer or cancer treatment. Dr. Efstathiou states “the best bladder you will ever have is the one you were born with (even if it has had an aggressive TURBT and some radiation)”.
Superficial recurrences can be managed conservatively, as 25% of patients will have non-muscle invasive tumors after complete response to TMT, including 60% recurrence-free after TURBT and BCG. Salvage cystectomy is feasible for those that progress to MIBC and rates are ~15%. Dr. Efstathiou also highlights that TMT is noted as an option (alongside radical cystectomy) by the NCCN guidelines and is advocated for as an option by advocacy groups such as BCAN.
In a recently published paper from Dr. Efstathiou’s group in European Urology, there are initial studies supporting biomarkers that may predict who may benefit from TMT4. This study found that signatures of T-cell activation and interferon gamma signaling were associated with improved DSS in a TMT cohort (HR 0.30, 95%CI 0.14-0.65), but not in the neoadjuvant chemotherapy and radical cystectomy cohort. Conversely, a stromal signature was associated with worse DSS in the neoadjuvant chemotherapy and radical cystectomy cohort, but not in the TMT cohort.
Dr. Efstathiou concluded with several important messages advocating for TMT in MIBC:
In clinically matched patients, survival is comparable in the modern era
- 85% of contemporary patients keep their own bladder (better than continent diversion) and long-term QoL is good
- TMT is not a non-surgical treatment: maximal TURBT and salvage cystectomy are important components
- TMT is supported by numerous guidelines (NCCN, AUA/ASTRO, EAU)
- There is a need for multidisciplinary engagement
- Donat SM, Shabsigh A, Savage C, et al. Potential impact of postoperative early complications on the timing of adjuvant chemotherapy in patients undergoing radical cystectomy: A high-volume tertiary cancer center experience. Eur Urol 2009 Jan;55(1):177-185.
- Giancalone NJ, Shipley WU, Clayman RH, et al. Long-term outcomes after bladder-preserving tri-modality therapy for patients with muscle-invasive bladder cancer: An updated analysis of the Massachusetts General Hospital. Eur Urol 2017 Jun;71(6):952-960.
- Kulkarni GS, Hermanns T, Wei Y, et al. Propensity score analysis of radical cystectomy versus bladder-sparing trimodal therapy in the setting of a multidisciplinary bladder cancer clinic. J Clin Oncol 2017;35(20):2299-2305.
- Efstathiou JA, Mouw KW, Gibb EA, et al. Impact of immune and stromal infiltration on outcomes following bladder-sparing trimodality therapy for muscle-invasive bladder cancer. Eur Urol 2019 Jan 31 [Epub ahead of print].
Massachusetts General Hospital, Boston, MA
Written By: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA
Further Related Content:
Opposing Argument: Radical Cystectomy is the Best Option for Muscle-Invasive Bladder Cancer