(UroToday.com) The 2026 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Mohammad Ganyani discussing the prognostic value of PSA nadir <= 0.2 ng/mL in metastatic hormone sensitive prostate cancer (mHSPC). The treatment landscape for mHSPC has evolved substantially with the adoption of early treatment intensification using androgen receptor pathway inhibitors (ARPIs) and chemotherapy in addition to ADT. PSA nadir has historically served as an important prognostic marker; existing thresholds were primarily established in ADT-only cohorts and may not accurately reflect outcomes in the contemporary combination-therapy era. Emerging evidence suggests that achieving a PSA nadir ≤0.2 ng/mL is associated with improved disease control and survival outcomes in patients with mHSPC. As such, Dr. Ganyani and colleagues conducted a systematic review and meta-analysis to evaluate the prognostic significance of PSA nadir ≤0.2 ng/mL in patients with mHSPC.
A systematic search of PubMed, Cochrane Library, and ClinicalTrials.gov was conducted through October 31, 2025. Randomized and prospective studies reporting outcomes by PSA nadir category in patients with HSPC were included. Eligible studies evaluated patients treated with ADT alone or in combination with ARPIs and/or chemotherapy. Reported hazard ratios for time to event outcomes stratified by PSA nadir ≤0.2 ng/mL were extracted and pooled for meta-analysis. The primary endpoint was overall survival, while secondary endpoints included radiographic progression free survival, PSA progression free survival, and time to castration resistance/hormone resistance. Publication bias was assessed using Begg’s and Egger’s tests.
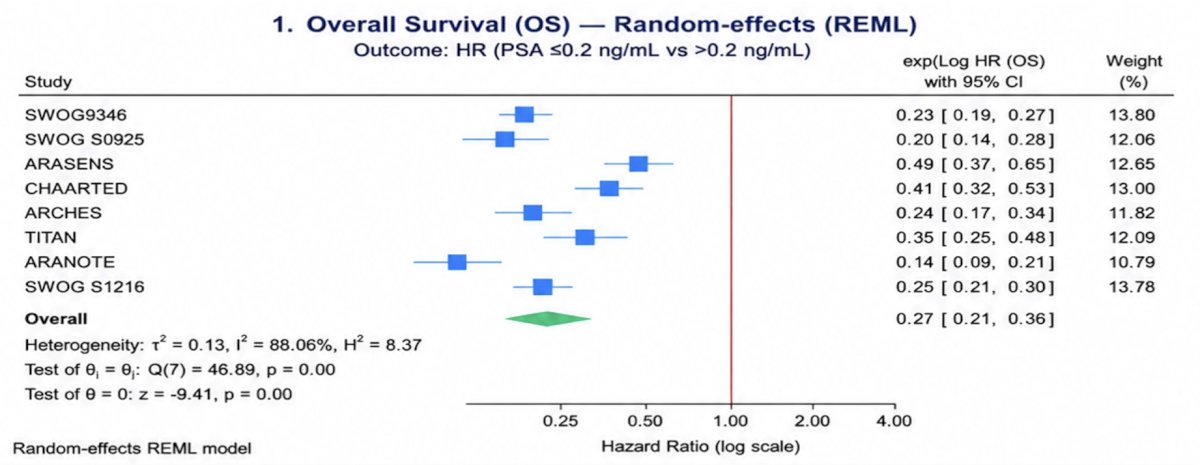
There were 8 trials comprising 6,582 patients included. Achieving a PSA nadir ≤0.2 ng/mL was associated with significantly improved overall survival, with a pooled HR of 0.27 (95% CI: 0.21–0.36; I² = 88.1%):
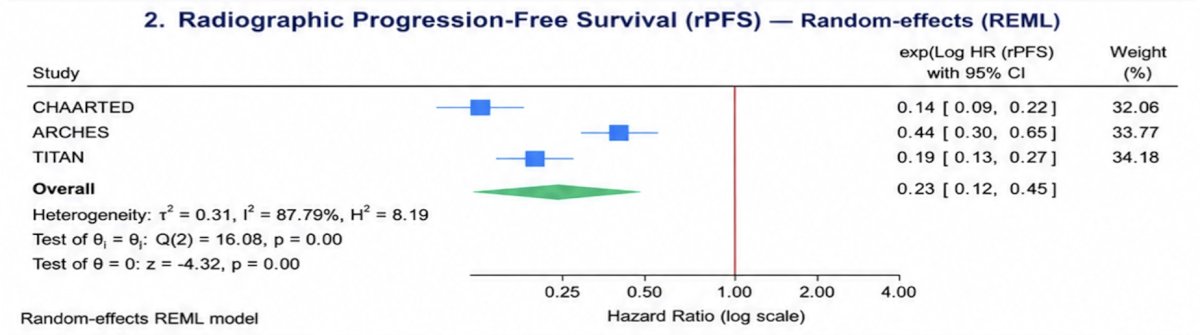
Consistent benefits were observed across secondary endpoints, including radiographic progression free survival (HR 0.23; 95% CI: 0.12–0.45; I² = 87.8%),
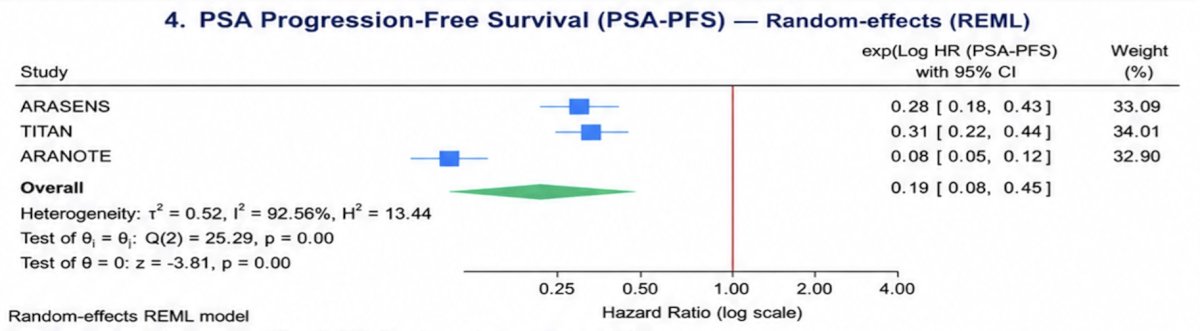
PSA progression free survival (HR 0.19; 95% CI: 0.08–0.45; I² = 92.6%),
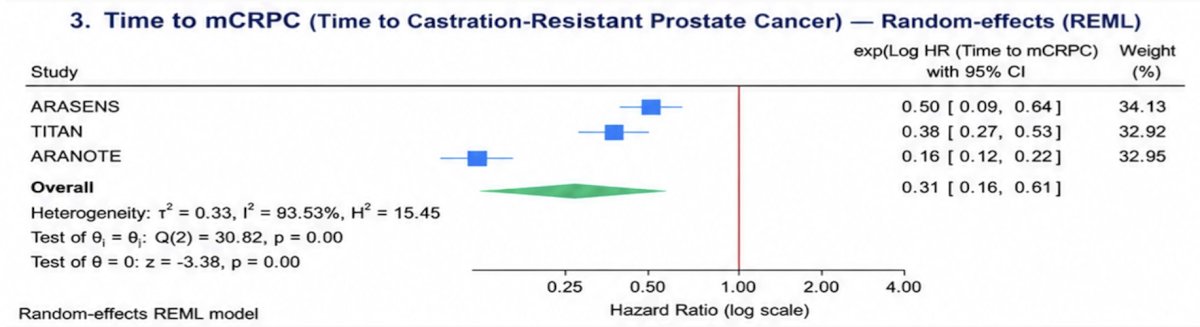
and delayed onset of hormone resistance (HR 0.31; 95% CI: 0.16–0.61; I² = 93.5%):
Begg’s and Egger’s tests showed no significant evidence of small-study effects across endpoints.
Dr. Ganyani concluded his presentation discussing the prognostic value of PSA nadir <= 0.2 ng/mL in mCSPC with the following take home points:
- Across contemporary mHSPC studies, achieving a PSA nadir ≤0.2 ng/mL was consistently associated with improved survival outcomes, prolonged disease control, and delayed progression to castration resistant disease
- These findings suggest that a deep PSA response may serve as a clinically meaningful and readily available prognostic marker in patients receiving modern systemic therapy
- PSA nadir may help support risk stratification and inform future treatment intensification or de-intensification strategies in routine clinical practice, particularly when accompanied by no radiographic evidence of disease progression
Presented by: Mohammad Arfat Ganyani, MBBS, Miami Cancer Institute, Baptist Health South Florida, Miami, FL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026