(UroToday.com) The 2026 ASCO annual meeting featured a prostate cancer trials in progress session and a presentation by Dr. Michael Ong discussing TRIPLE-SWITCH (SWOG/CCTG-PR26), a randomized phase III clinical trial for the addition of docetaxel to androgen receptor pathway inhibitors (ARPIs) in patients with metastatic castration sensitive prostate cancer (mCSPC) and suboptimal PSA response.
Management of patients with mCSPC remains a challenge due to its incurable nature and heterogeneous response to ADT and ARPIs. Recent analyses of phase III ADT + ARPI trials show that mCSPC with suboptimal PSA response (≥0.2 ng/ml at 6-12 months) have a poor prognosis, short time to castration-resistance (CRPC), and a 30-36 month median overall survival.
While docetaxel could also be utilized in mCSPC, there is equipoise about its use in ARPI-treated patients because of (i) an absence of randomized data for docetaxel in this setting, (ii) the toxicity of docetaxel with impact on quality of life for patients, and (iii) the selection of docetaxel treatment by disease volume rather than disease biology. CCTG-PR26 (TRIPLE-SWITCH) is a joint CCTG-SWOG trial run through the NCI National Clinical Trials Network. This study investigates whether adding docetaxel prior to the development of CRPC, regardless of disease volume, will improve overall survival in ARPI-treated mCSPC patients who show evidence of suboptimal response.
This international, open-label, randomized phase III trial compares standard ADT + ARPIs against the addition of docetaxel to ADT + ARPIs in mCSPC patients with suboptimal PSA response, defined as PSA ≥0.2 ng/mL after 6-12 months of ADT and ≥4 months of ARPIs. Stratification will be based on PSA levels, ARPI type, presence of liver metastasis, disease recurrence status, and time since ADT initiation.
Arm 1 will continue standard ADT + ARPIs (abiraterone acetate with prednisone, apalutamide, enzalutamide or darolutamide). Arm 2 will receive docetaxel 75mg/m2 IV every 3 weeks for up to 6 cycles in addition to continuing standard ADT + ARPIs:
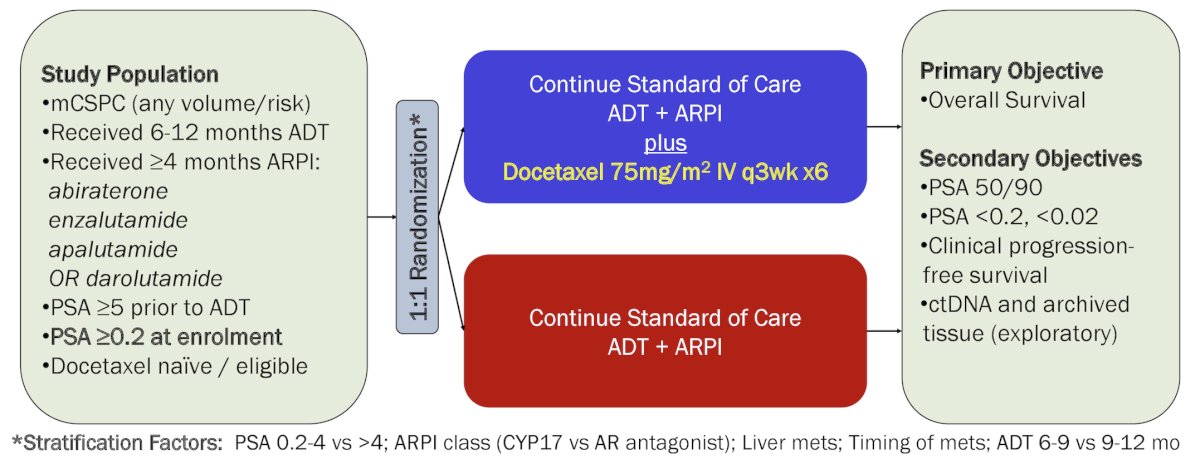
The sample size is 830 patients in order to detect a targeted 33% improvement in overall survival (hazard ratio 0.75) using a 1-sided 0.025 level test with 85% power. Key eligibility criteria are:
- ≥18 years
- Histologically confirmed prostate adenocarcinoma
- Metastatic disease present and confirmed by conventional imaging (CT and/or bone scan)
- PSA ≥5.0 ng/mL prior to ADT
- Receipt of ADT for 6-12 months and ARPI for ≥4 months
- PSA ≥0.2 ng/mL within 14 days of enrolment
- Adequate organ and marrow function
- ECOG performance status 0-2
- Eligible for docetaxel chemotherapy
- No evidence of disease progression or biochemical progression on ADT prior to enrolment
The primary endpoint is overall survival, and secondary endpoints include PSA response, PSA kinetics, and clinical progression-free survival. Correlative studies will explore the prognostic and predictive value of circulating tumor DNA and the association between molecular signatures in primary prostate cancer tissue and clinical outcomes.
Enrolment has been initiated in January 2025 and is ongoing.
Presented by: Michael Ong, MD, The Ottawa Hospital Cancer Centre, Ottawa, Ontario, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026