(UroToday.com) The 2026 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Kenshiro Shiraishi discussing 10 year follow-up results from a prospective study of mpMRI-guided salvage radiotherapy with lesion-directed dose escalation after radical prostatectomy. Salvage radiotherapy after radical prostatectomy has traditionally been delivered as uniform dose distribution of the prostate bed without lesion visualization. Previously, Dr. Shiraishi and colleagues prospectively implemented an image-guided salvage strategy integrating high-resolution multiparametric MRI (mpMRI) and lesion-directed dose escalation. At the ASCO 2026 annual meeting, Dr. Shiraishi reported the long-term oncologic outcomes of this pioneering approach.
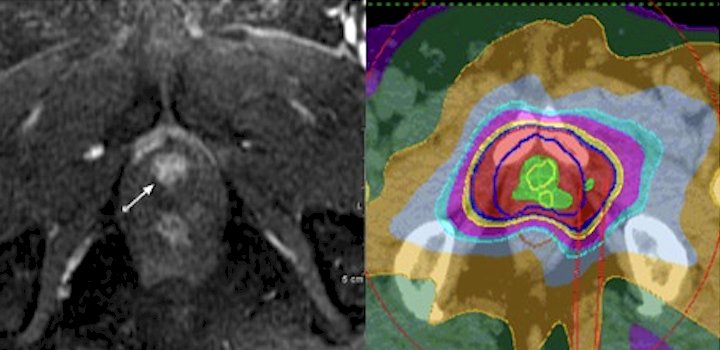
This prospective, single-arm clinical study was registered in the UMIN database in 2013. Patients with biochemical recurrence (PSA ≥0.2 ng/mL) after radical prostatectomy and no evidence of distant metastasis were enrolled. All patients underwent 3T mpMRI with an endorectal coil prior to salvage radiotherapy. When a focal recurrent lesion was identified, intensity modulated radiotherapy (IMRT) with simultaneous integrated boost was delivered:
- 70 Gy to the MRI-defined lesion
- 66 Gy to the prostate bed in 33 fractions
Patients without visible lesions received prostate-bed irradiation alone. Long-term clinical outcomes were analyzed:
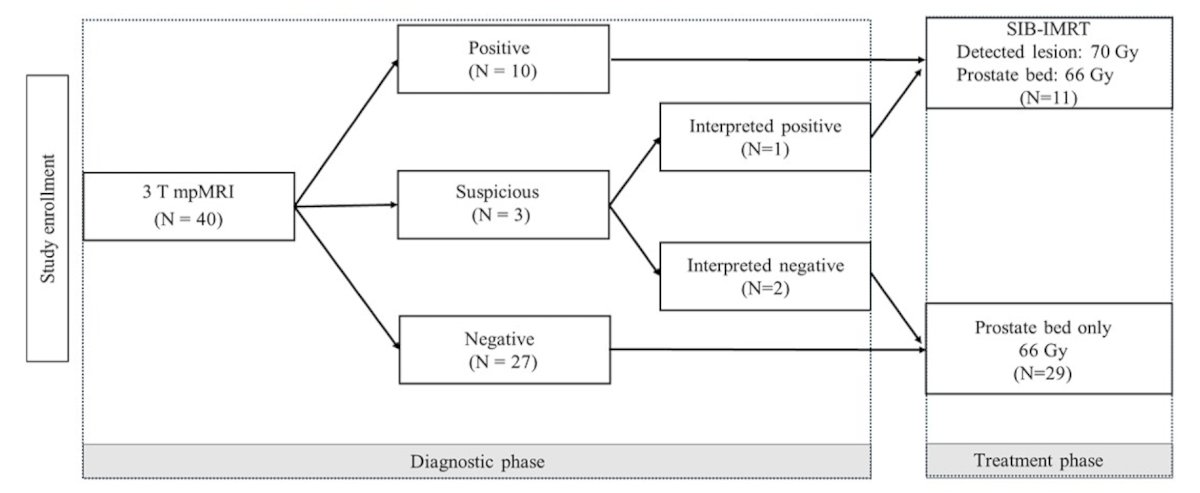
A total of 40 patients completed protocol treatment, with a median PSA of 0.25 ng/mL. mpMRI identified focal recurrence sites in 11 patients (27.5%), all of whom received lesion-directed simultaneous integrated boost-IMRT:
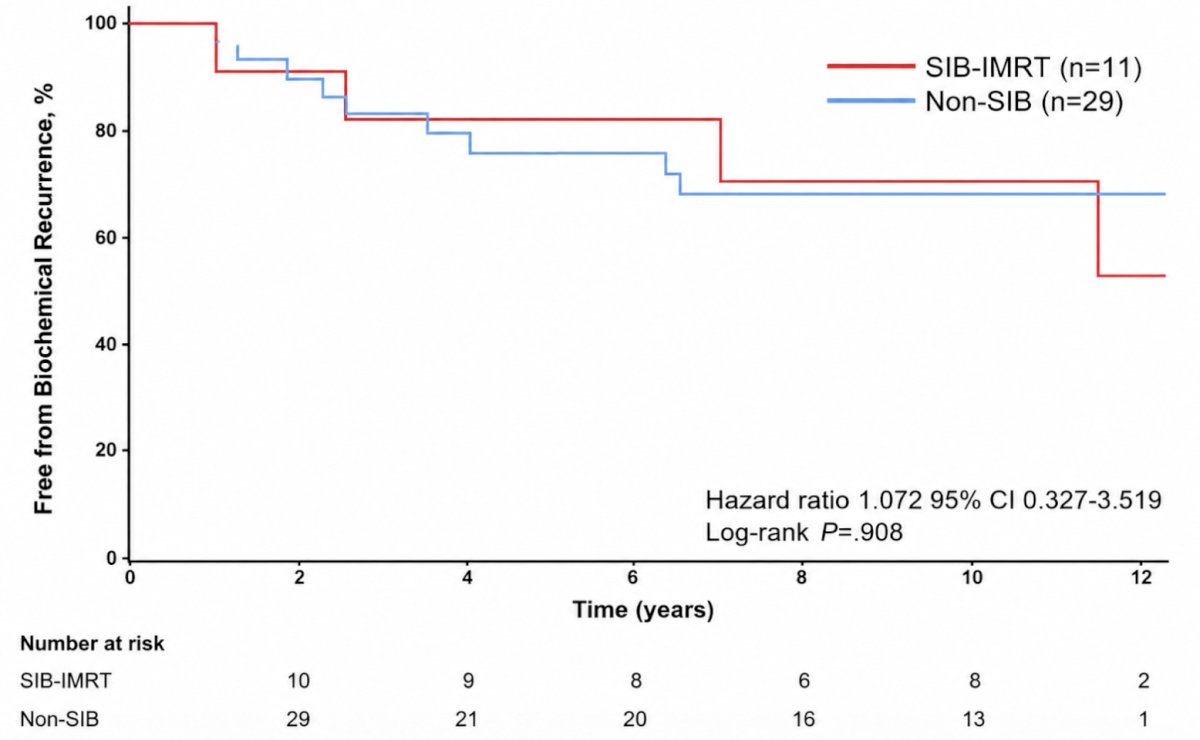
After a median follow-up of 10.6 years, treatment failure occurred in 13 patients (32.5%).
Among patients treated with simultaneous integrated boost-IMRT, 4 of 11 developed biochemical recurrence, whereas among 29 patients without mpMRI-detectable recurrence, 9 developed biochemical recurrence (HR 1.072, 95% CI 0.327-3.519):
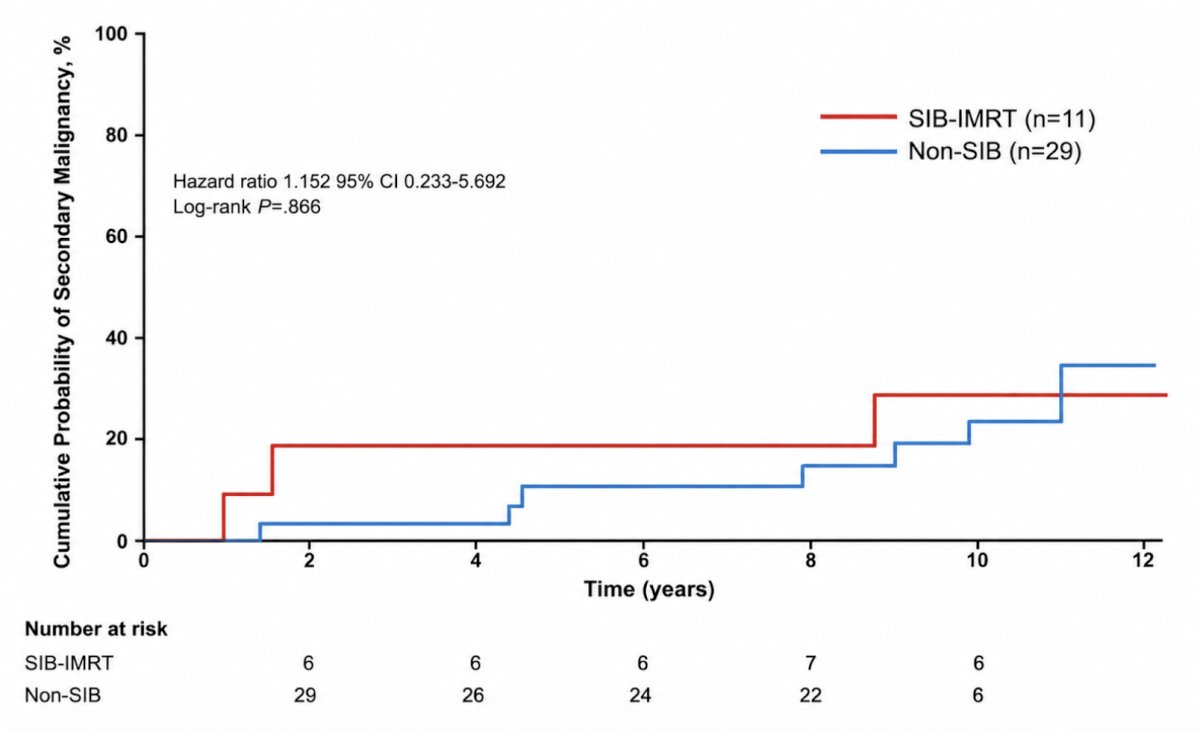
Importantly, no patient developed radiologically evident local recurrence within the irradiated prostate bed, including those treated with simultaneous integrated boost in their disease course. Distant metastases developed in 3 patients, and 1 patient died from prostate cancer. Treatment-related adverse events were considered acceptable. One patient without simultaneous integrated boost experienced grade 3 perforation of the sigmoid colon. Secondary malignancies were diagnosed in 10 patients (HR 1.152, 95% CI 0.233-5.692):
Dr. Shiraishi concluded his presentation discussing 10 year follow-up results from a prospective study of mpMRI-guided salvage radiotherapy with lesion-directed dose escalation after radical prostatectomy with the following take home points:
- With long-term follow-up, mpMRI-guided salvage radiotherapy achieved excellent durable local control. The absence of in-field local failures regardless of mpMRI detectability supports the biological and clinical validity of lesion-directed salvage intensification
- These findings underscore individualized a simultaneous integrated boost approach and highlight the need for future studies to refine patient selection and treatment intensification strategies in salvage settings, including ADT and/or elective pelvic nodal irradiation
- Future research:
- Failures is not local → driven by occult extraprostatic disease
- Supports image-guided + risk-adapted strategy by next-generation imaging, including PSMA-PET
Presented by: Kenshiro Shiraishi, Teikyo University School of Medicine, Tokyo, Japan
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026