(UroToday.com) The 2026 ASCO annual meeting featured an optimizing care for patients with metastatic castration resistant prostate cancer (mCRPC) session and a presentation by Dr. Louise Emmett discussing how to better personalize treatment with 177Lu-PSMA-617. How stringent should patient selection criteria be?
In the TheraP trial,1 tumors required an SUVmax ≥20 at >1 one site, SUV ≥10 at all measurable lesions, and the absence of FDG-positive/PSMA-negative mismatch disease. These stringent criteria resulted in a 28% screening failure rate. In contrast, VISION2 required only a single lesion demonstrating uptake above liver background activity and resulted in a lower screening failure rate of 13%.
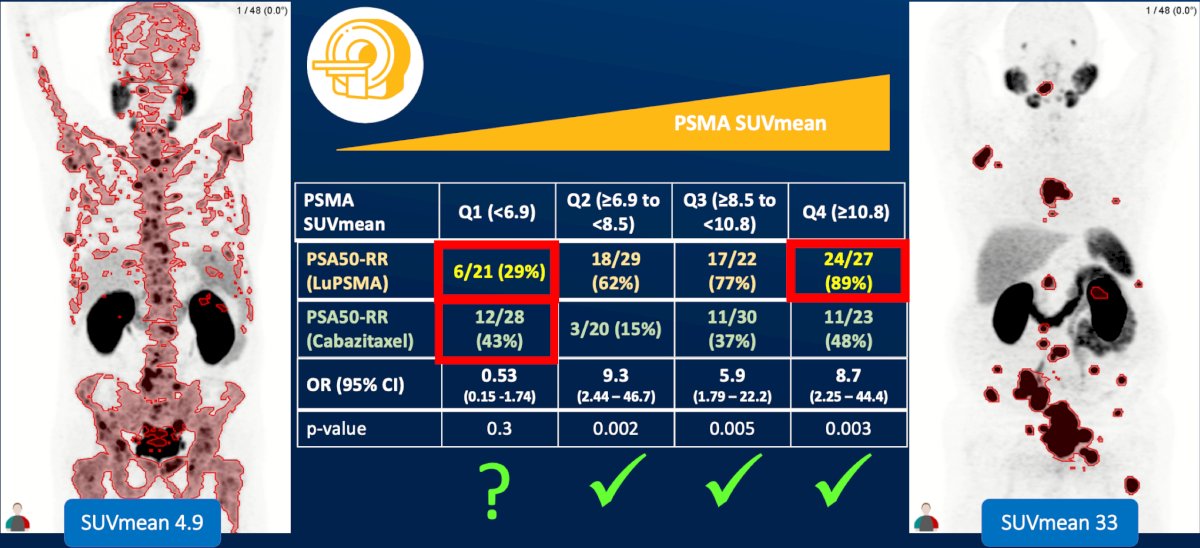
Dr. Emmett then discussed quantitative PET metrics and whether a lower threshold of PSMA expression exists below which response to 177Lu-PSMA therapy is essentially impossible. There is emerging evidence evaluating SUVmean as a potentially more informative biomarker than traditional SUVmax measurements. Can SUVmean identify patients that will not benefit from PSMA-targeted therapy?
CtDNA looks like a good predictor of response for radioligand therapy based on work from TheraP. Kwon et al3 assessed prostate cancer driver genes across 290 serial plasma cell-free DNA samples from 180 molecular imaging-selected patients with mCRPC.6 A low (ctDNA <2%) pretreatment ctDNA fraction predicted a superior progression-free survival and overall survival compared to higher (ctDNA 2-30% and >30%) pretreatment ctDNA fractions:
![CtDNA looks like a good predictor of response for radioligand therapy based on work from TheraP. Kwon et al3 assessed prostate cancer driver genes across 290 serial plasma cell-free DNA samples from 180 molecular imaging-selected patients with mCRPC [6]. A low (ctDNA <2%) pretreatment ctDNA fraction predicted a superior progression-free survival and overall survival compared to higher (ctDNA 2-30% and >30%) pretreatment ctDNA fractions:](/images/com-doc-importer/271-asco-2026/asco-2026-how-to-better-personalize-treatment-with-177lu-psma-617/image-1.jpg)
Data evaluating PSMA total tumor volume (TTV) demonstrated important interactions between disease burden and treatment benefit. In patients in ENZA-p4 receiving enzalutamide + 177Lu-PSMA-617, those with PSMA TTV <234 mL achieved a median overall survival of 35 months compared with 28 months among patients with PSMA TTV >234 mL (HR 0.23, 95% CI: 0.13–0.42; p < 0.00001). In the enzalutamide alone arm, median overall survival was 39 months for patients with PSMA TTV <234 mL and 20 months for those with PSMA TTV >234 mL (HR 0.66, 95% CI 0.36-1.21; p = 0.18). Importantly, the interaction test was statistically significant (p = 0.008), suggesting that tumor volume may influence the magnitude of benefit derived from radioligand therapy:
![Data evaluating PSMA total tumor volume (TTV) demonstrated important interactions between disease burden and treatment benefit. In patients in ENZA-p [4] receiving enzalutamide + 177Lu-PSMA-617, those with PSMA TTV <234 mL achieved a median overall survival of 35 months compared with 28 months among patients with PSMA TTV >234 mL (HR 0.23, 95% CI: 0.13–0.42; p < 0.00001). In the enzalutamide alone arm, median overall survival was 39 months for patients with PSMA TTV <234 mL and 20 months for those with PSMA TTV >234 mL (HR 0.66, 95% CI 0.36-1.21; p = 0.18). Importantly, the interaction test was statistically significant (p = 0.008), suggesting that tumor volume may influence the magnitude of benefit derived from radioligand therapy:](/images/com-doc-importer/271-asco-2026/asco-2026-how-to-better-personalize-treatment-with-177lu-psma-617/image-2.jpg)
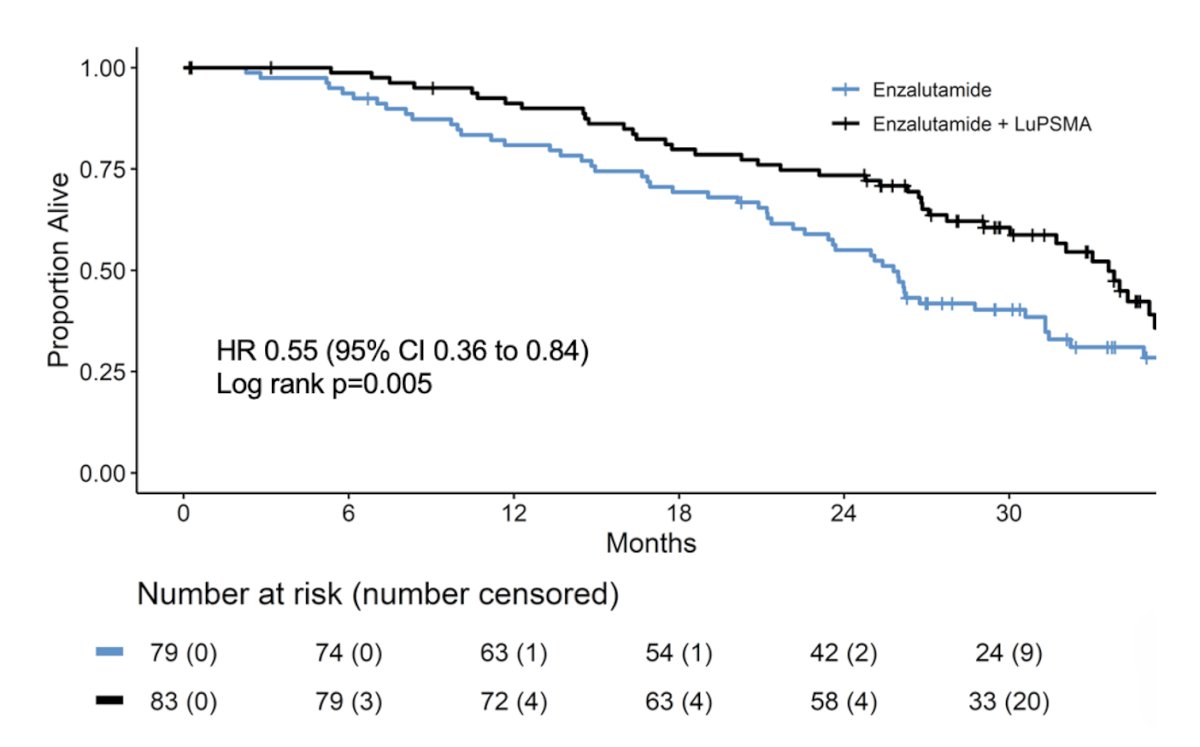
Dr. Emmett also addressed whether ARPIs should routinely be combined with PSMA-targeted radioligand therapy. Looking further at the ENZA-p trial evaluating enzalutamide with or without 177Lu-PSMA-617, ENZA-p demonstrated a significant overall survival advantage for combination therapy. The median overall survival was 34 months (95% CI: 30–37) with enzalutamide + 177Lu-PSMA-617 versus 26 months (95% CI: 23–31) for enzalutamide alone (HR 0.549, 95% CI 0.36–0.84; log-rank p = 0.0053):
Published earlier in 2026, Emmett et al.5 evaluated the predictive value of early PSMA upregulation for the response to enzalutamide +/- 177Lu-PSMA-617 among patients in ENZA-p. Notably, 68% of patients had a rise in SUVmean after 15 days of enzalutamide:
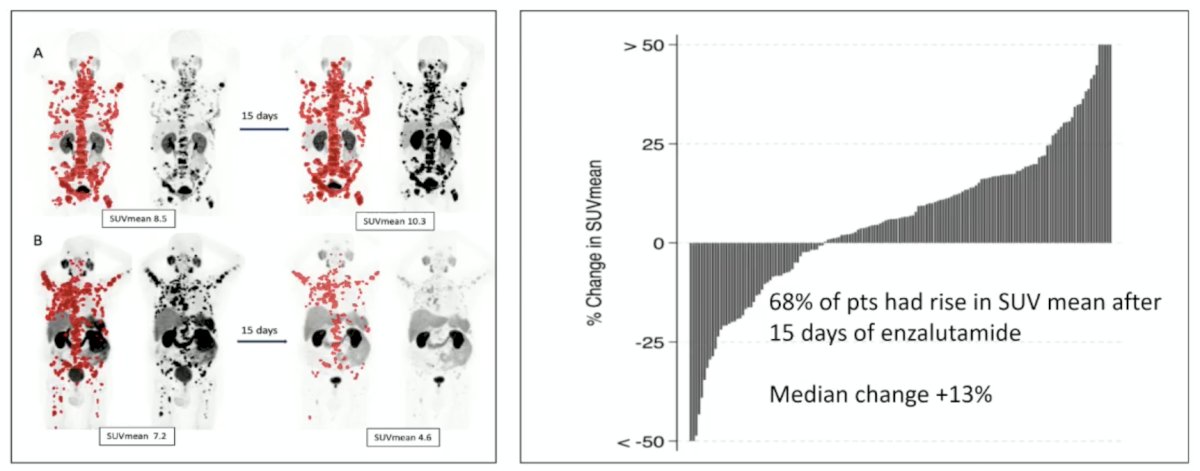
These findings provide mechanistic support for combining androgen receptor blockade with PSMA-targeted radioligand therapy and may partially explain the efficacy observed in ENZA-p.
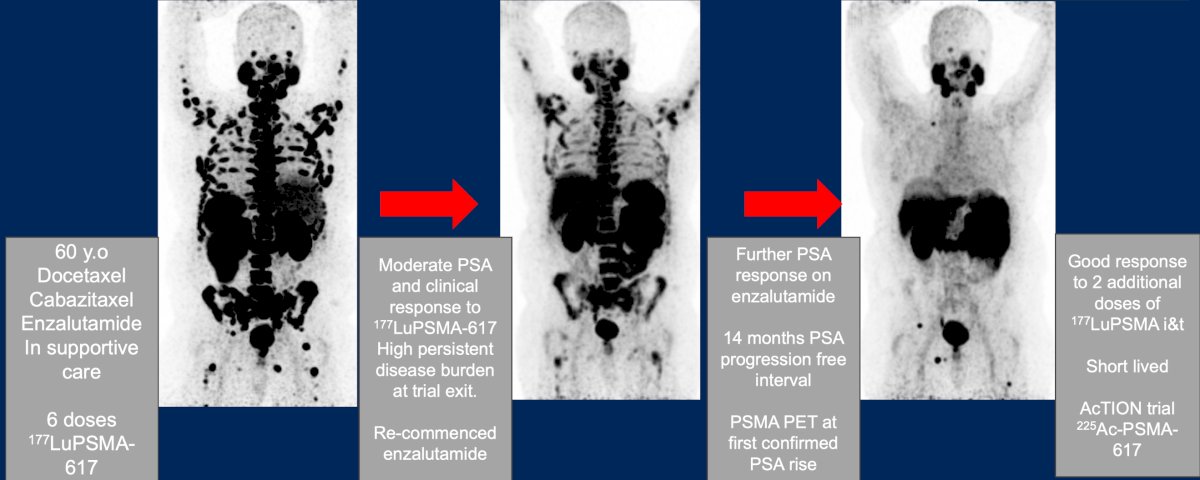
The role of ARPI rechallenge in conjunction with radioligand therapy was further explored through a clinical case presentation. A 60-year-old patient who had previously received docetaxel, cabazitaxel, and enzalutamide underwent six doses of 177Lu-PSMA-617, achieving a moderate PSA and clinical response but maintaining substantial residual disease burden at treatment completion. Upon restarting enzalutamide, the patient experienced an additional PSA response and achieved a 14-month PSA progression-free interval. Subsequent PSMA PET imaging at PSA progression demonstrated renewed sensitivity to additional radioligand therapy, with two further doses of 177Lu-PSMA-I&T producing another clinical response. The patient was ultimately enrolled in the AcTION trial for 225Ac-PSMA-617:
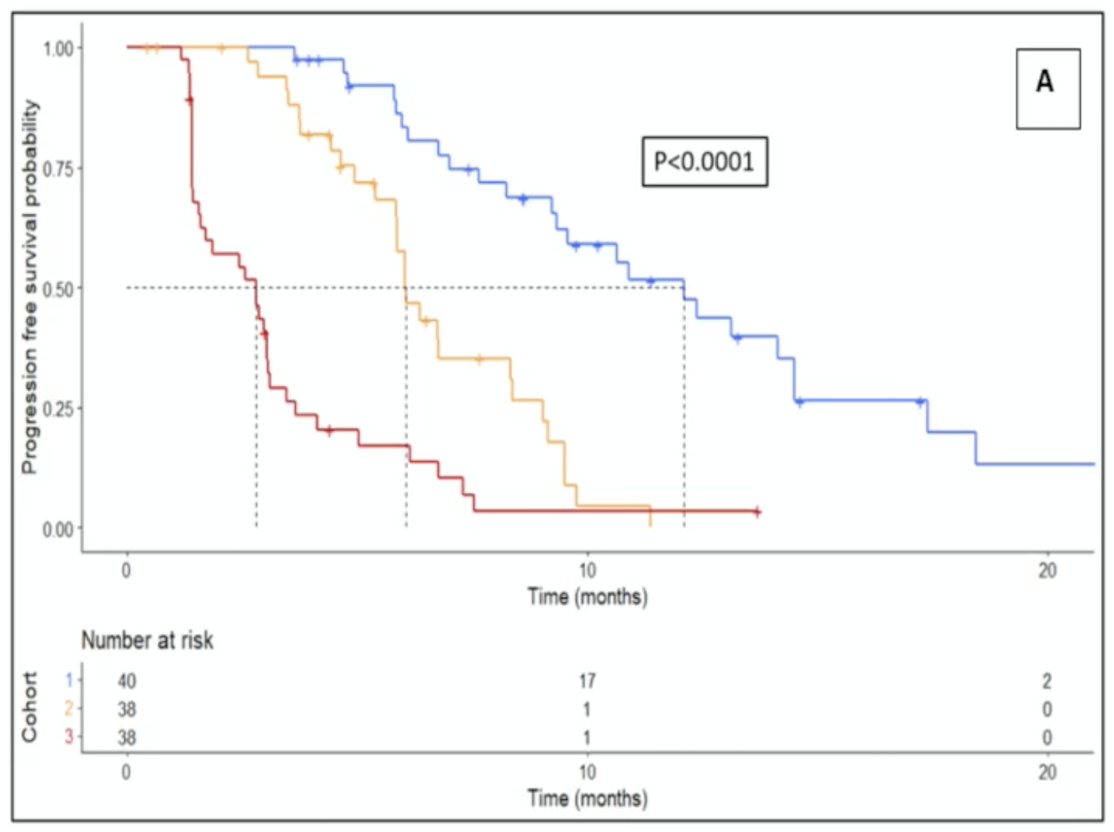
Dr. Emmett emphasized that better dynamic biomarkers are needed to identify radiation-sensitive and radiation-resistant disease early in treatment. Such biomarkers could allow clinicians to distinguish meaningful responses from early resistance and personalize treatment intensity accordingly. The ENZA-p imaging biomarker program recently assessed baseline and week-6 SPECT/CT imaging in 81 patients receiving 177Lu-PSMA-617.6 Combining PSA responses with changes in PSMA tumor volume provided superior prognostic information compared with either marker alone and improved prediction of overall survival. Among 71 evaluable patients, 12 achieved a complete PSMA-TTV response (blue), 34 patients achieved a PSA decline exceeding 90% without a complete PSMA-TTV response (black), and 25 patients demonstrated neither a marked PSA nor imaging response (red):
Notably, 75% of patients with a PSA decline greater than 90% did not achieve a corresponding marked reduction in PSMA tumor volume, underscoring the limitations of relying solely on PSA measurements.
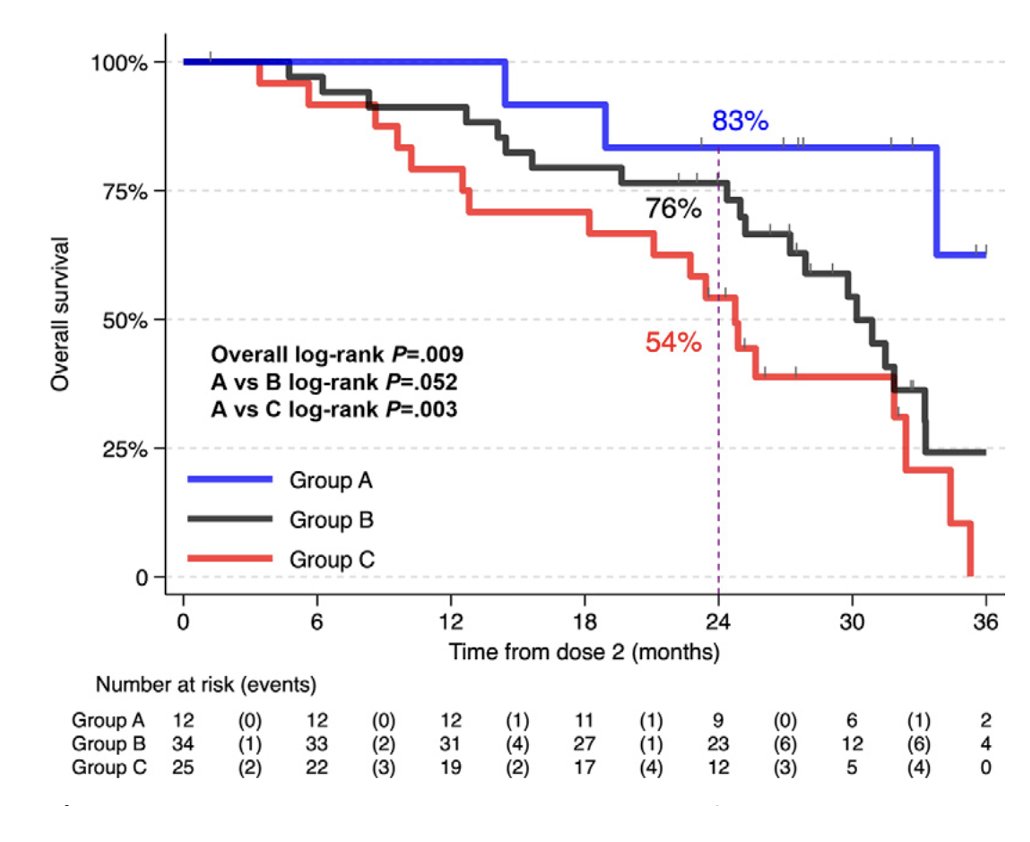
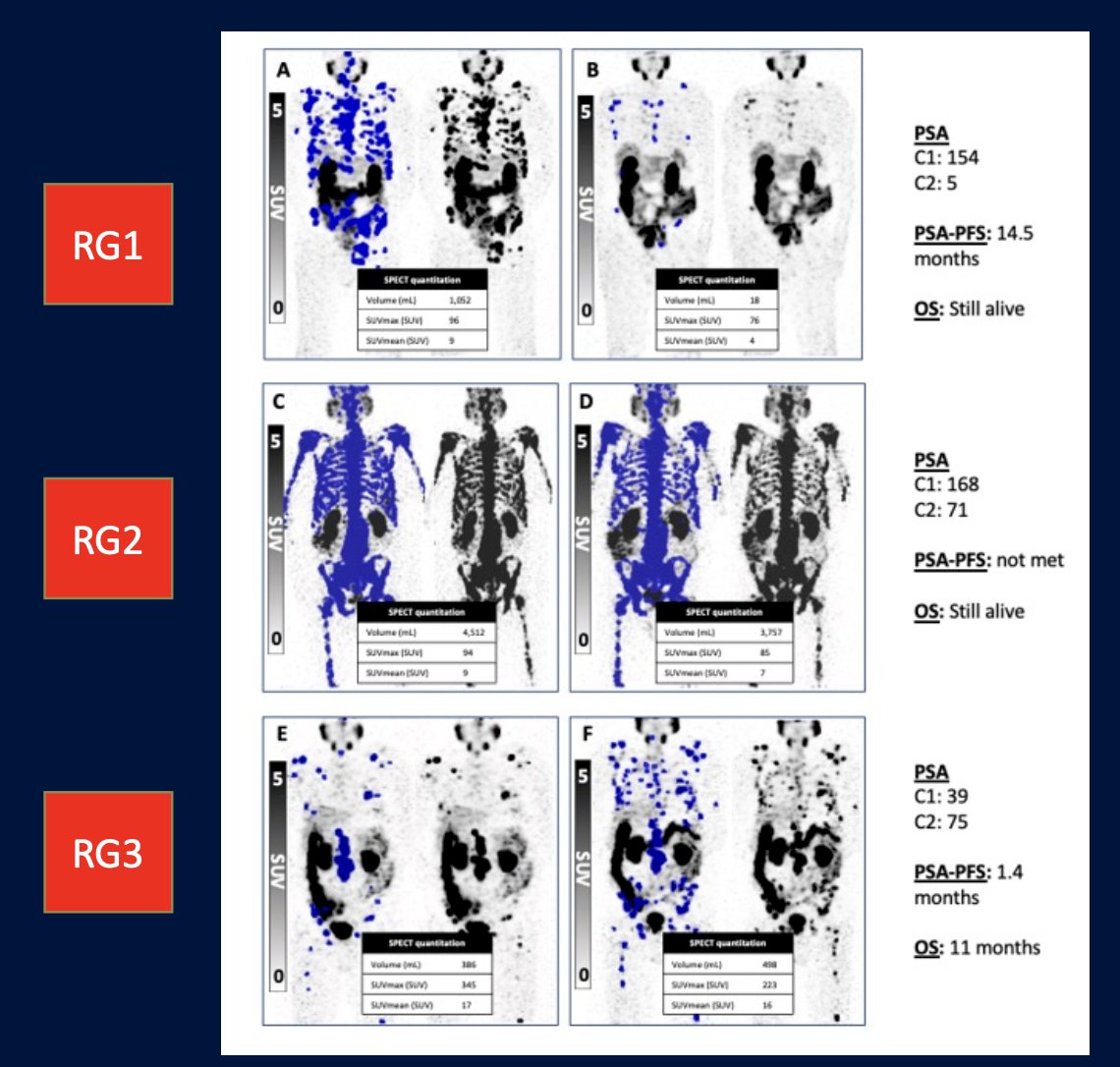
In 2023, Dr. Emmett and colleagues reported results of their study evaluating progression-free survival and overall survival based on treatment interval adjustment utilizing 177LuPSMA 24-hour SPECT/CT and early PSA response.7 There were 125 men treated with 6 times weekly 177LuPSMA-I&T doses (median 3 cycles, IQR 2-4) at a median dose of 8.0 GBq (95% CI 7.5-8.0). Following dose 2 (week 6), a composite PSA and 177LuPSMA 24-hour SPECT/CT imaging response determined ongoing management:
- Response Group 1 (marked reduction in PSA/imaging partial response): break in treatment until subsequent PSA rise, then re-treatment
- Response Group 2 (stable or reduced PSA and/or imaging stable disease): 6-weekly treatments until six doses, or no longer clinically benefiting
- Response Group 3 (rise in PSA and/or imaging progressive disease): recommend alternative treatment
The results were as follows:
- Response Group 1: progression-free survival 12.3 months, overall survival 22 months, treatment break for 6 months
- Response Group 2: progression-free survival 6.2 months, overall survival 15 months, no treatment break
- Response Group 3: progression-free survival 2.8 months, overall survival 11 months, early more to alternative treatment
Taken together, re-treatment with 177Lu-PSMA-617 at PSA rise after treatment pause had a PSA50 response rate range of 37-73%.
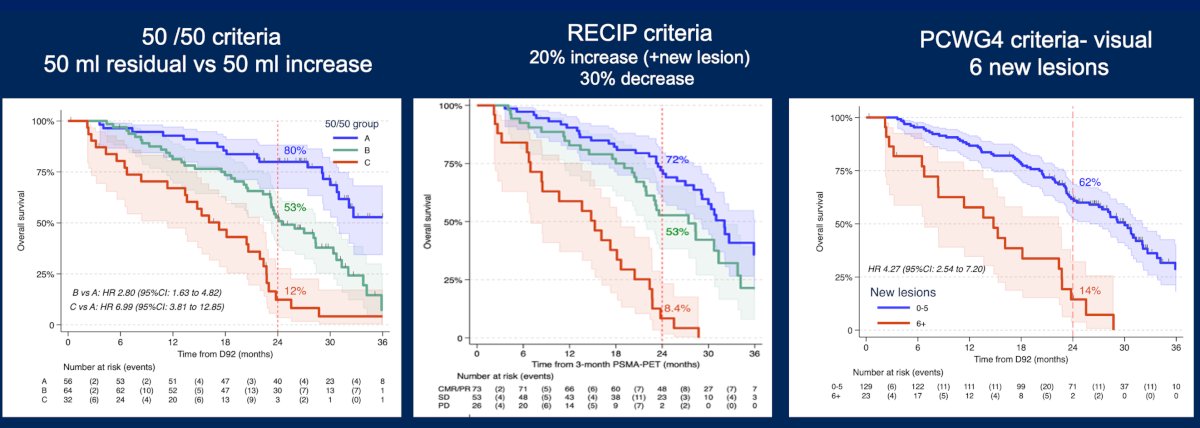
With regards to emerging PSMA PET response criteria, there is data from ENZA-p demonstrating that disease progression identified on three-month PSMA PET imaging is strongly prognostic for limited two-year survival regardless of the response criteria employed. This observation was consistent across visual assessment methods, 50/50 criteria, residual tumor volume approaches, and RECIP criteria. Importantly, progression detected on PSMA PET remained prognostically independent of the specific measurement methodology utilized:
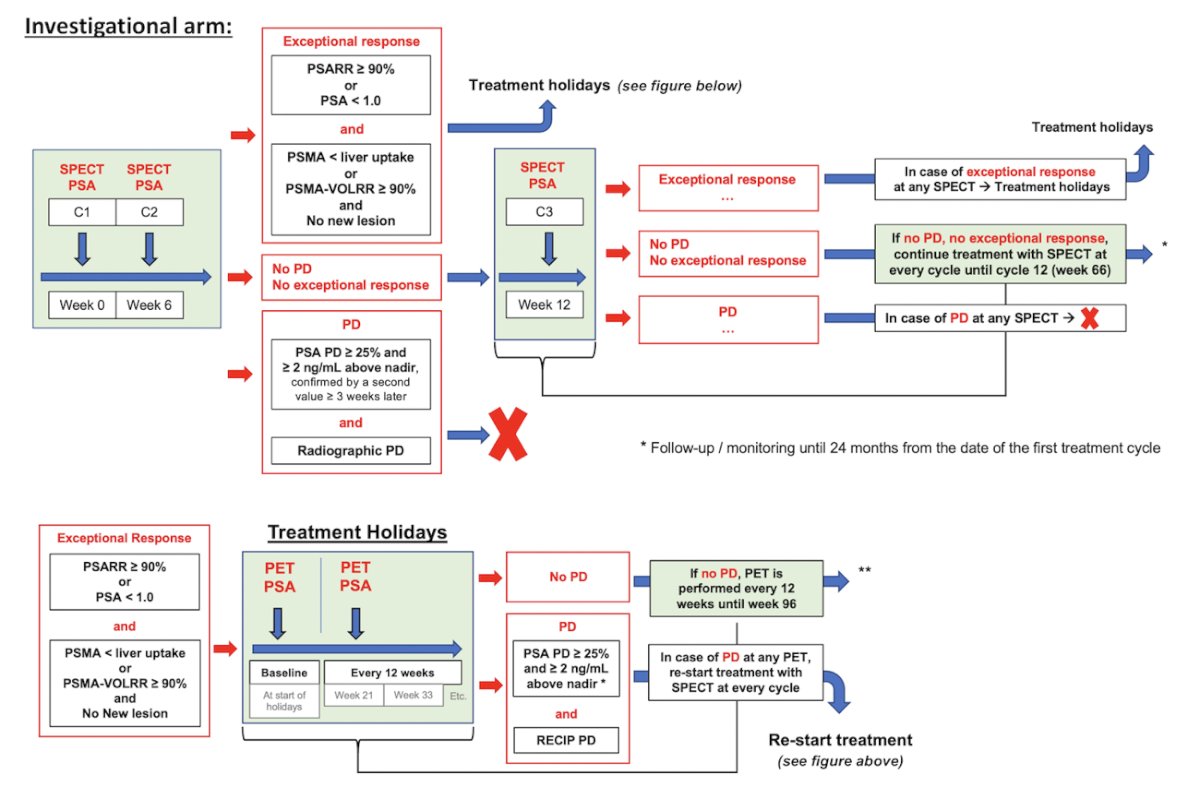
Several ongoing trials are attempting to operationalize these concepts into clinical practice. The FLEX-MRT trial is an investigator-initiated prospective phase 2, open-label, randomized, controlled, parallel group, single-center trial. The aim is to assess the 2-year survival rate in mCRPC patients treated with a flexible dosing schedule of 177Lu-PSMA radiopharmaceutical therapy up to 12 cycles in comparison to the fixed dosing schedule of 6 cycles. Patients with progressive mCRPC post-androgen receptor pathway inhibitor and post-taxane-based chemotherapy are eligible for the PSMA PET VISION trial criteria. The overview of the study design is as follows:
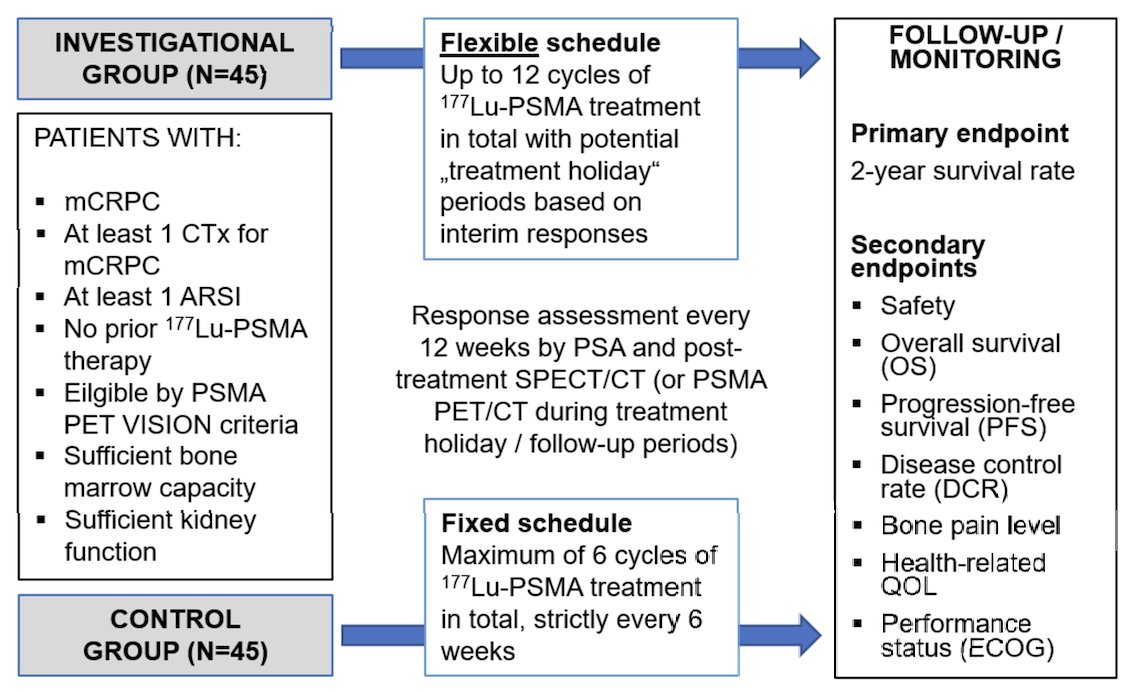
Imaging response to radiopharmaceutical therapy is assessed using 177Lu-PSMA-617 SPECT/CT after each cycle and PSMA PET/CT during treatment holidays (every 12 weeks), respectively. In the investigational arm, radiopharmaceutical therapy will be restarted after a treatment holiday if the patient experiences a ≥25% PSA progression and an imaging progression according to the RECIP:
The primary endpoint is the 2-year survival rate calculated from the date of the first cycle of radiopharmaceutical therapy.
The OPTIMAL-PSMA randomized phase II trial aims to determine the safety and efficacy of a dosing regimen comprised of an intense induction followed by a maintenance period of 177Lu-PSMA-597 therapy, compared to standard of care 6 doses weekly in men with mCRPC. Part A in the figure below visually demonstrates the induction sequence (Days 1, 3, and 15) followed by extended-interval maintenance dosing. In contrast, the control arm receives standard 7.4 GBq dosing every 6 weeks for six cycles:
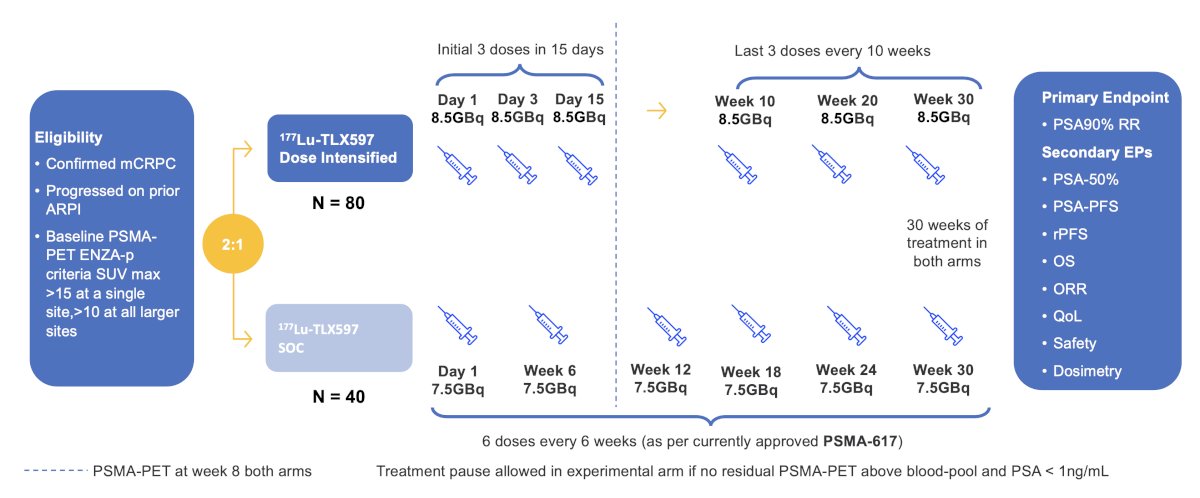
The primary endpoint is PSA50 response.
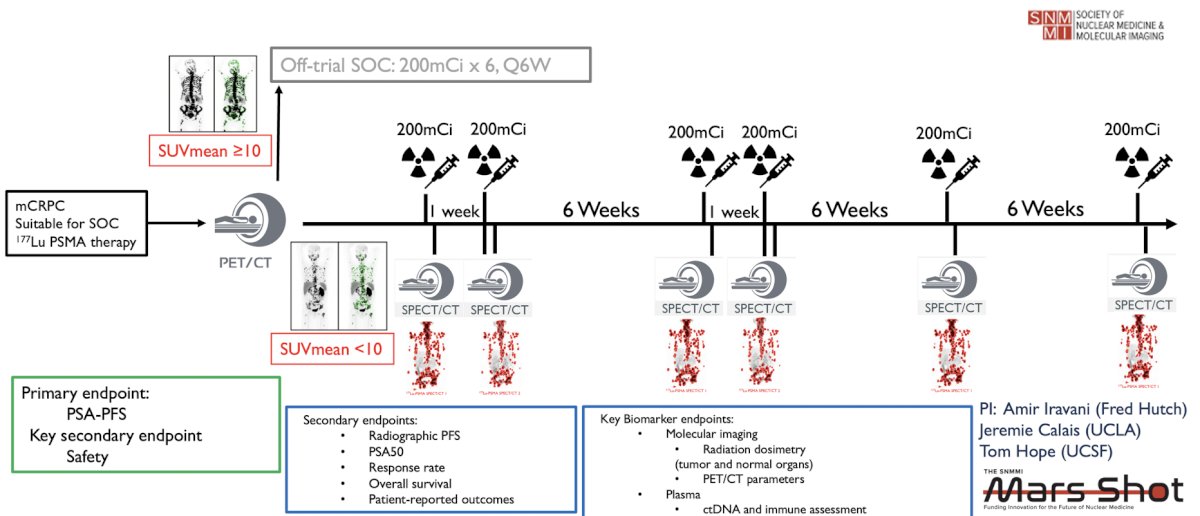
As part of intensifying treatment up front, Dr. Emmett also highlighted biomarker-modulated PSMA theranostics (NCT0656299), whereby low PSMA mCRPC patients are treatment intensified with 177Lu-PSMA-617:
Future rational combination strategies and potential partners for PSMA-targeted radioligand therapy, including:
- Immune checkpoint inhibitors
- T-cell engagers
- Cancer vaccines
- CAR-T cell therapies
- Alpha-emitting radionuclides such as 223Ra, 225Ac, 212Pb, and 211At
- Androgen receptor-targeted therapies
- PARP inhibitors
- DNA damage response inhibitors
- Chemotherapy
- Antibody-drug conjugates directed against PSMA, STEAP1/2, or B7-H3
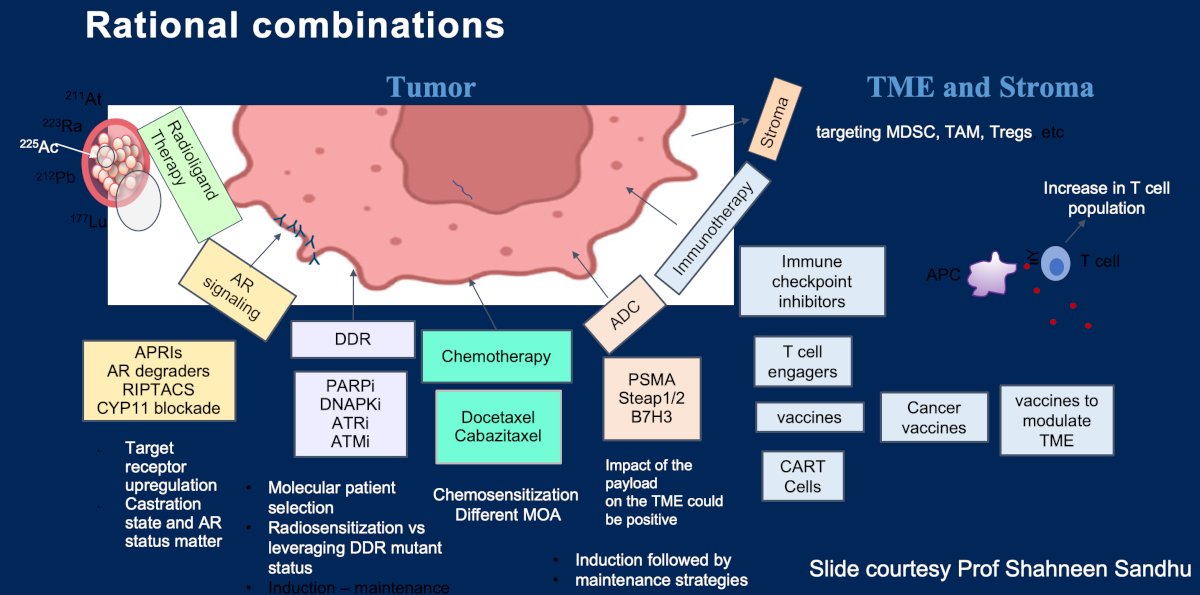
Dr. Emmett emphasized that the optimal combination should accomplish several objectives simultaneously: complementary targeting of distinct tumor clones, avoidance of additive toxicity, generation of biologic synergy, and improved durability of response. Understanding tumor microenvironment interactions, androgen receptor biology, DNA damage repair pathways, and radiosensitization mechanisms will be critical to the successful development of these strategies.
Dr. Emmett concluded her presentation discussing how to better personalize treatment with 177Lu-PSMA-617 with the following take-home points:
- Screening PSMA PET can be used more effectively to avoid treatment in patients guaranteed not to respond, thereby minimizing opportunity cost and toxicity
- While the addition of ARPI to PSMA-targeted therapy is biologically attractive and supported by encouraging clinical data, additional evidence remains necessary
- Biomarker-guided therapy, adaptive dosing approaches, and rational combination strategies are poised to become the cornerstone of personalized PSMA-targeted radioligand therapy for patients with mCRPC
Presented by: Louise Emmett, MD, MBChB, FRACP, FAANMS, Professor, Director of Theranostics and Nuclear Medicine, St. Vincent’s Hospital Sydney, University of New South Wales, Sydney, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Kwan EM, Ng SWS, Tolmeijer SH, et al. Lutetium-177-PSMA-617 or cabazitaxel in metastatic prostate cancer: circulating tumor DNA analysis of the randomized phase 2 TheraP trial. Nat Med. 2025 Aug;31(8):2722-2736.
- Emmett L, Papa N, Subramaniam S, et al. Prognostic and predictive value of baseline PSMA-PET total tumour volume and SUVmean in metastatic castration-resistant prostate cancer in ENZA-p (ANZUP1901): A substudy from a multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Sep;26(9):1168-1177.
- Emmett L, Swiha M, Papa N, et al. Predictive value of early PSMA upregulation for the response to enzalutamide +/- 177Lu-PSMA-617 in poor-risk, metastatic, castration-resistant prostate cancer: Substudy of the randomized, phase 2 ENZA-p trial. Nat Cancer. 2026 Apr;7(4):622-630.
- Ayati N, Papa N, Crumbaker M, et al. 177Lu-PSMA-617 SPECT/CT for early prediction of overall survival in participants with metastatic castration-resistant prostate cancer. Radiology. 2026 Apr;319(1):e252672.
- Emmett L, John N, Pathmanandavel S, et al. Patient outcomes following a response biomarker-guided approach to treatment using 177Lu-PSMA-I&T in men with metastatic castrate-resistant prostate cancer (Re-SPECT). Ther Adv Med Oncol. 2023 Mar 1:15:17588359231156392.