(UroToday.com) The 2026 ASCO annual meeting featured an optimizing care for patients with metastatic castration resistant prostate cancer (mCRPC) session and a presentation by Dr. Biren Saraiya discussing early integration of palliative and supportive care. To frame the discussion, Dr. Saraiya first defined palliative care, which is specialized medical care for people living with serious illness and is focused on the relief of suffering.
Palliative care is delivered by a multidisciplinary team and addresses multiple domains of patient well-being. Primary palliative care is delivered by the patient's primary clinical team—including oncologists, cardiologists, and primary care physicians—and specialist or secondary palliative care is delivered by professionals specifically trained in palliative care, including physicians, advanced practice providers, nurses, social workers, and chaplains.
Expanding upon this framework, Dr. Saraiya reviewed the domains of palliative care outlined in the National Consensus Project Clinical Practice Guidelines. These domains include:
- Physical aspects of care, such as pain, nausea, and vomiting
- Psychological concerns, including anxiety and depression
- Social support needs for patients and families
- Spiritual, religious, and existential concerns
- Cultural considerations
- Ethical and legal aspects of care
These domains are addressed throughout the disease trajectory, including at the end of life. Indeed, there is substantial overlap between palliative care and oncology. Oncologic care itself is specialized medical care for individuals living with cancer and is likewise focused on relief of suffering, whether or not a cure remains achievable. Modern cancer care already relies on multidisciplinary and interdisciplinary teams that include medical oncologists, radiation oncologists, urologic oncologists, advanced practice providers, nurses, pharmacists, social workers, financial counselors, and patient navigators. Thus, integration of palliative care should not be viewed as a separate process, but rather as an extension of comprehensive cancer care.
Dr. Saraiya highlighted updated ASCO Clinical Practice Guidelines and multiple studies demonstrating that integration of palliative care into routine oncologic care improves quality of life, improves mood, decreases chemotherapy utilization near the end of life when patients have a more accurate understanding of prognosis, and may improve survival. These observations have been replicated across multiple randomized studies and healthcare settings. To further illustrate the concept, Dr. Saraiya presented the palliative care continuum. Historically, palliative care was often viewed as a service primarily reserved for end-of-life care. Contemporary models instead emphasize integration beginning at diagnosis and continuing throughout the disease course. Curative therapies, disease-modifying interventions, palliative interventions, hospice care, and bereavement support are no longer viewed as isolated phases but rather as overlapping components of longitudinal patient care: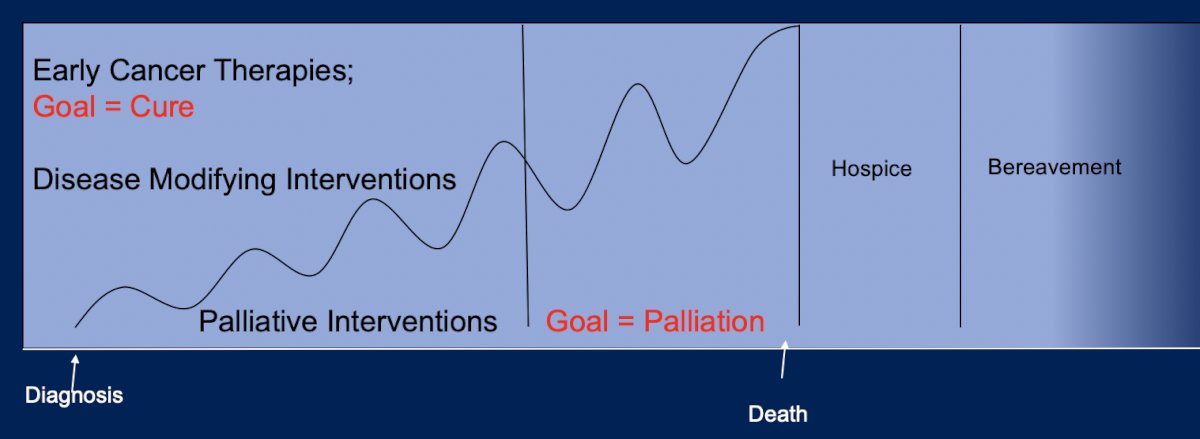
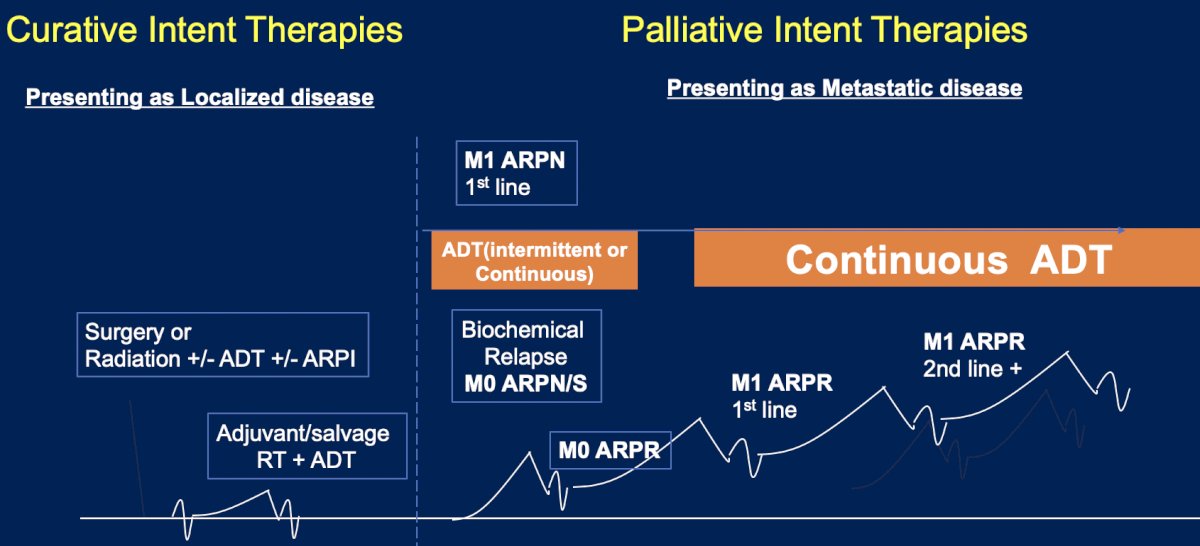
Dr. Saraiya then applied this framework specifically to prostate cancer. Patients presenting with localized disease may undergo surgery, radiation therapy, ADT, and androgen receptor pathway inhibitors (ARPIs) with curative intent. However, as the disease progresses through biochemical recurrence, non-metastatic castration-resistant disease, metastatic hormone-sensitive disease, and ultimately metastatic castration-resistant prostate cancer (mCRPC), treatment goals progressively shift toward palliation. Dr. Saraiya emphasized that while therapies continue to prolong survival, many treatments administered in advanced disease settings are fundamentally palliative in nature:
This concept is particularly relevant when discussing contemporary treatment options for mCRPC. Patients may receive ARPIs, chemotherapy, PARP inhibitors, radioligand therapies, immunotherapies, and clinical trial interventions. Although these therapies provide meaningful clinical benefit, they are associated with a broad range of adverse effects, including hormonal toxicities, fatigue, cytopenias, xerostomia, gastrointestinal toxicities, neurologic toxicities, and organ dysfunction. As a result, symptom management becomes increasingly important throughout the treatment journey.
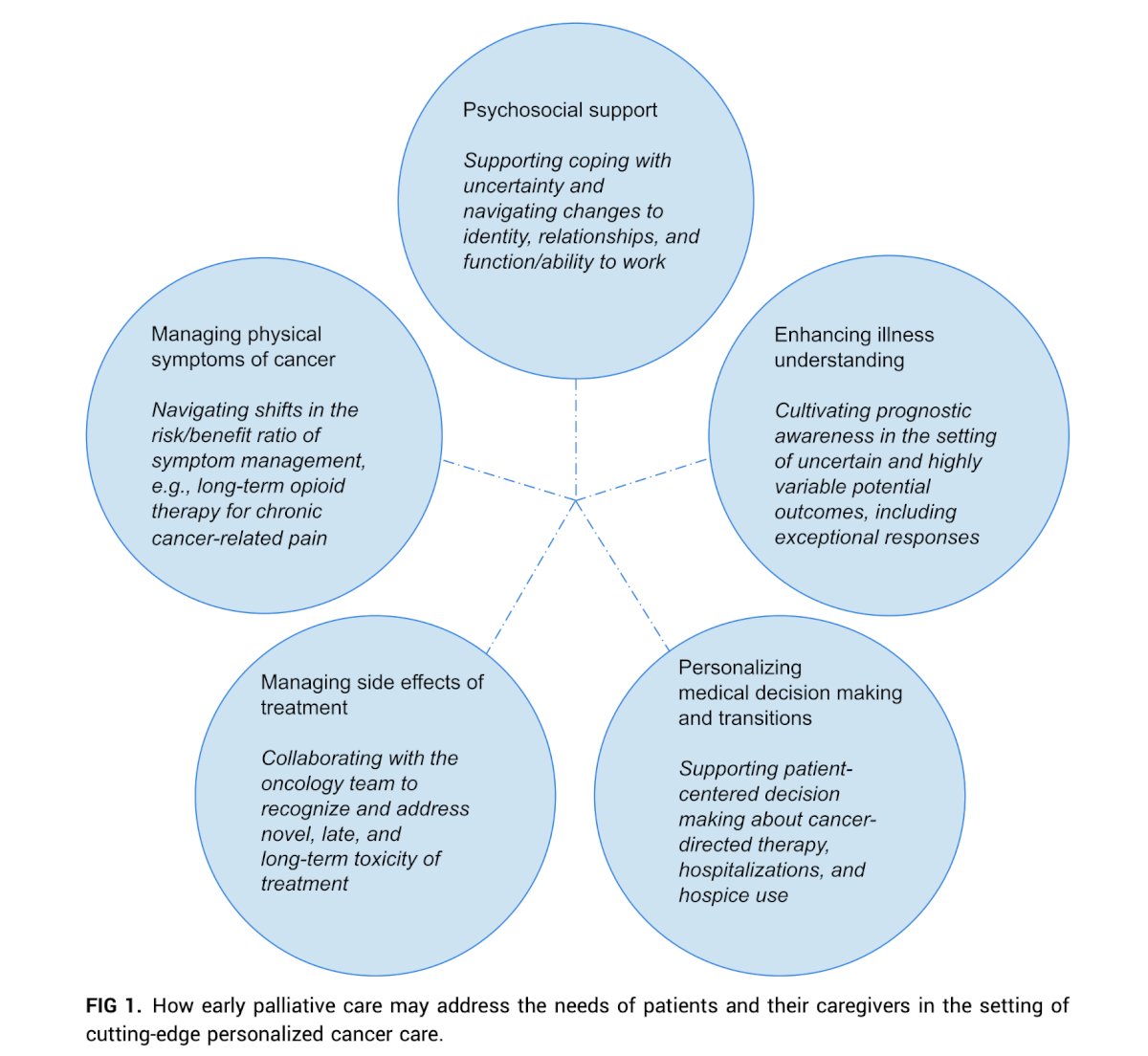
Why should palliative care be integrated into mCRPC management? By definition, the primary goal of treatment in mCRPC is palliation. Furthermore, patients frequently experience symptoms requiring active management. Beyond symptom burden, patients require psychosocial support, assistance with illness understanding, and guidance regarding increasingly complex treatment decisions. Petrillo and colleagues1 demonstrated that integration of early palliative care improves quality of life, reduces symptom intensity, and facilitates communication regarding illness and prognosis. While overall survival benefits have been inconsistently demonstrated across studies, the improvements in patient-centered outcomes remain compelling. Potential palliative care interventions include structured communication about prognosis, systematic symptom assessment and management, support for coping strategies, and routine longitudinal follow-up:
The second half of the presentation focused on practical implementation strategies. Dr. Saraiya acknowledged that implementation will vary substantially across practices depending on available resources. He encouraged clinicians to learn from successful integration models already established within their own cancer centers. For example, thoracic oncology programs frequently incorporate palliative care from the first visit for patients with metastatic disease. Similarly, practices can learn from colleagues working in rural settings, single-specialty groups, or resource-limited environments. Implementation tools include systematic symptom inventories such as the NCCN Distress Thermometer, regimented symptom assessment pathways, electronic medical record-based triggers, standardized order sets, and workflow modifications designed to facilitate referrals. Although guidelines may recommend universal approaches, practical implementation must be adapted to local resources. Accordingly, practices should evaluate available palliative care personnel, develop referral triggers, establish workflows, and create systems that can function within their specific healthcare environment.
Dr. Saraiya proposes creating an inventory of available palliative care resources across domains, including physical symptoms, psychological symptoms, and social concerns. Practices should determine which needs can be addressed by physicians, advanced practice providers, nurses, social workers, or chaplains within the oncology team and identify areas where secondary palliative care support may be required. Available resources may include onsite palliative care programs, remote or telemedicine services, or stand-alone palliative care clinics. Understanding the local resource landscape is an essential first step before designing referral pathways.
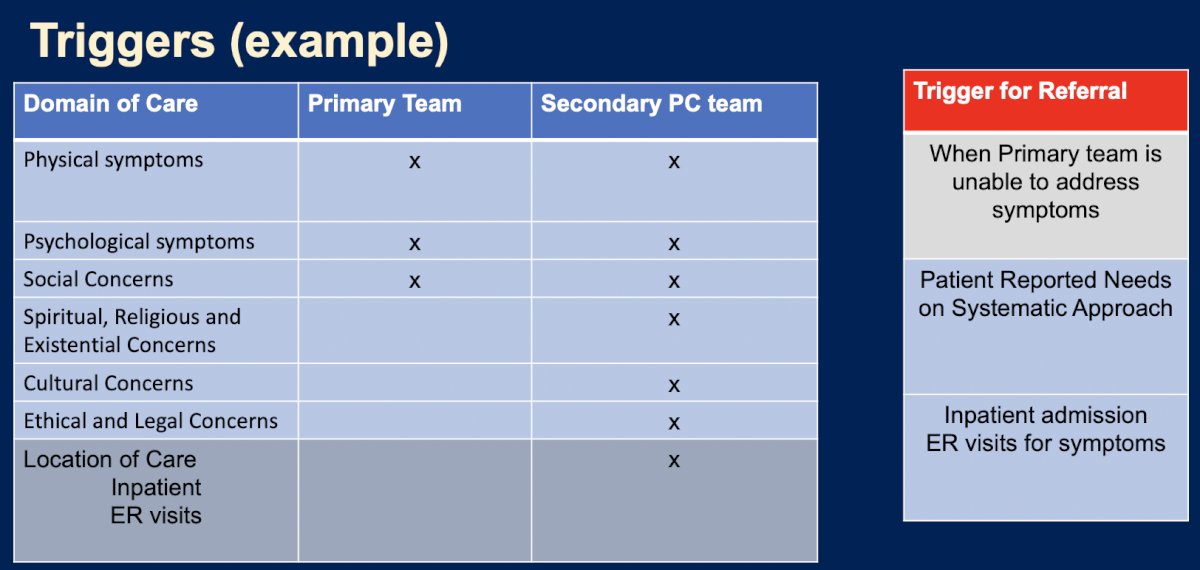
There are several practical referral triggers, including physical symptoms, psychological concerns, and social needs, that may initially be managed by the primary oncology team but should trigger referral when symptoms become difficult to manage or exceed local expertise. Spiritual, religious, existential, cultural, ethical, and legal concerns often warrant direct involvement of specialist palliative care providers. Additional triggers may include inpatient admissions, emergency room visits for symptom management, and patient-reported needs identified through systematic screening programs:
There may be barriers to implementation, and access remains a significant challenge, particularly related to insurance coverage. There are ongoing advocacy efforts surrounding palliative care benefits for Medicaid patients, and legislation supporting expanded palliative care access has been enacted in several states, including California, Hawaii, Maine, Oregon, and New Jersey. Resource limitations and lack of expertise represent additional barriers. Potential solutions include telemedicine partnerships, development of internal expertise, and creation of standardized care pathways. Institutional buy-in can also be challenging, however implementation studies suggest that integrated palliative care models can be financially sustainable through increased clinical volume and associated reimbursement.
Finally, Dr. Saraiya outlined several practical approaches moving forward. At the practice level, clinicians should develop primary palliative care pathways and establish referral triggers for specialist consultation. At the institutional level, advocacy for palliative care resources remains essential, and referrals should be made whenever appropriate to sustain and grow palliative care programs. At the state level, continued advocacy for reimbursement and coverage expansion will be necessary. Across all levels, collaboration remains the cornerstone of improving care for patients with advanced prostate cancer.
Dr. Saraiya concluded this presentation discussing early integration of palliative and supportive care with the following take-home points:
- Early palliative care improves quality of life, symptom burden, coping, and patient satisfaction
- Every practice should develop a plan for integrating early palliative care into routine care based on available local resources
- Referral triggers should be established and may include diagnosis-based, symptom-based, and systems-based criteria
Presented by: Biren Saraiya, MD, Robert Wood Johnson Medical School, New Brunswick, NJ
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference:
- Petrillo LA, Jones KF, El-Jawahri A, et al. Why and How to Integrate Early Palliative Care into Cutting-Edge Personalized Cancer Care. Am Soc Clin Oncol Educ Book. 2024 Jun;44(3):e100038.