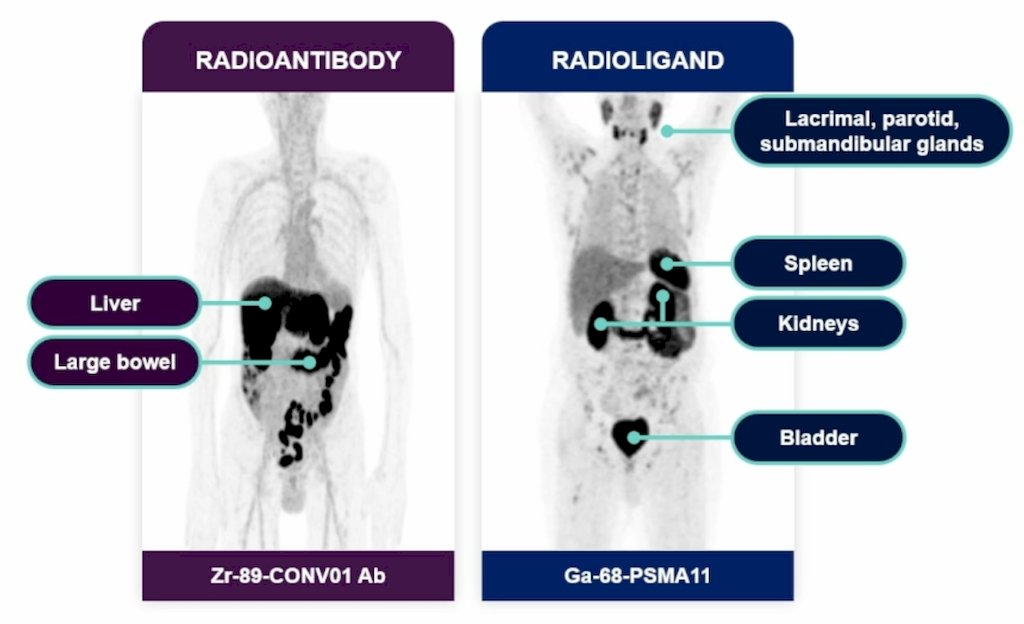
(UroToday.com) The 2026 ASCO annual meeting featured a radioligand innovation in prostate cancer session and a presentation by Dr. Michael Morris discussing CONVERGE-01 Part 3 assessing Ac-225 rosopatamab tetraxetan (CONV01-α) in 177Lu-PSMA-617 pretreated metastatic castration resistant prostate cancer (mCRPC). Dr. Morris emphasized that the biodistribution of antibodies versus small molecules for radioligand therapy leads to:
- Reduced uptake in the salivary glands and kidneys
- Uptake in the liver without clinical impact
- Longer elimination half-life with a potential hematologic impact
- Superior uptake and retention in tumor cells:
There are also advantages of Ac-225 as an alpha-emitting payload, including:
- A 10-day half-life that complements the antibody targeting moiety
- No need for restrictive lifestyle modification, and the decay daughters (Bi-213 and Fr-221) are rapidly cleared without toxicity
- Accelerator-derived production facilitates an adequate supply of radioisotopes
- High-purity production methodology eliminates complicated waste disposal/handling and long-term decay concerns
CONV01-α, an alpha-emitting radionuclide conjugated to a PSMA-targeting monoclonal antibody, has demonstrated safety and encouraging activity in prior investigator-initiated trials.1 This phase 2 multi-center CONVERGE-01 trial is evaluating the safety and efficacy of CONV01-α in patients with mCRPC, including those previously treated with Lu-PSMA-617 or -I&T (Lu-PSMA) in a dose escalation and in an initial expansion cohort.
Eligible patients for CONVERGE-01 had PSMA PET-positive (VISION criteria2) mCRPC with previous exposure to ≥1 ARPI, 0-1 taxane regimens, and 1-6 cycles of Lu-PSMA. CONV01-α was administered in a single cycle of two doses (D1 and D15). Dose escalation used a BOIN design protocol (dose levels: 45 and 55 kBq/kg, with optional initial expansion):
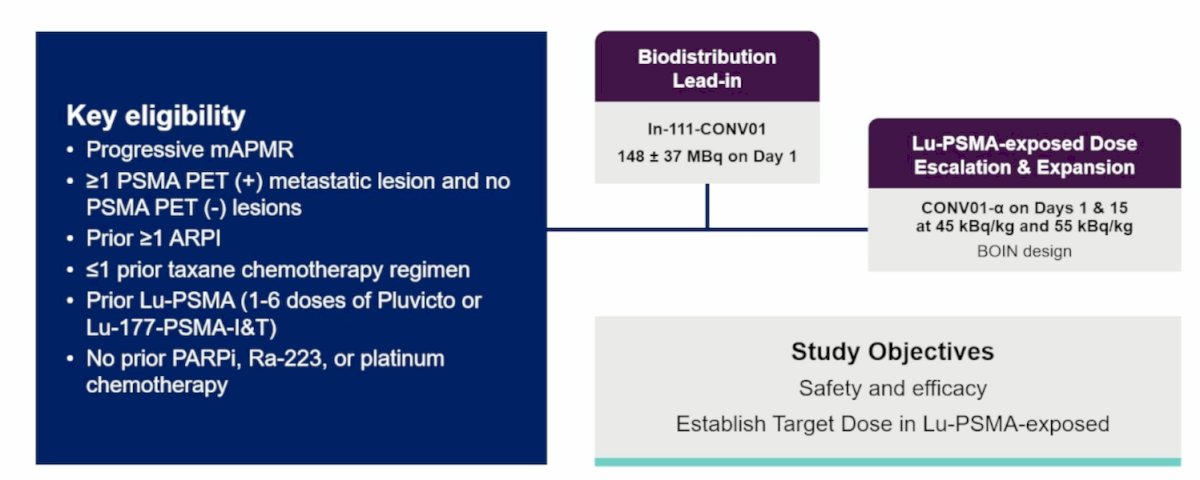
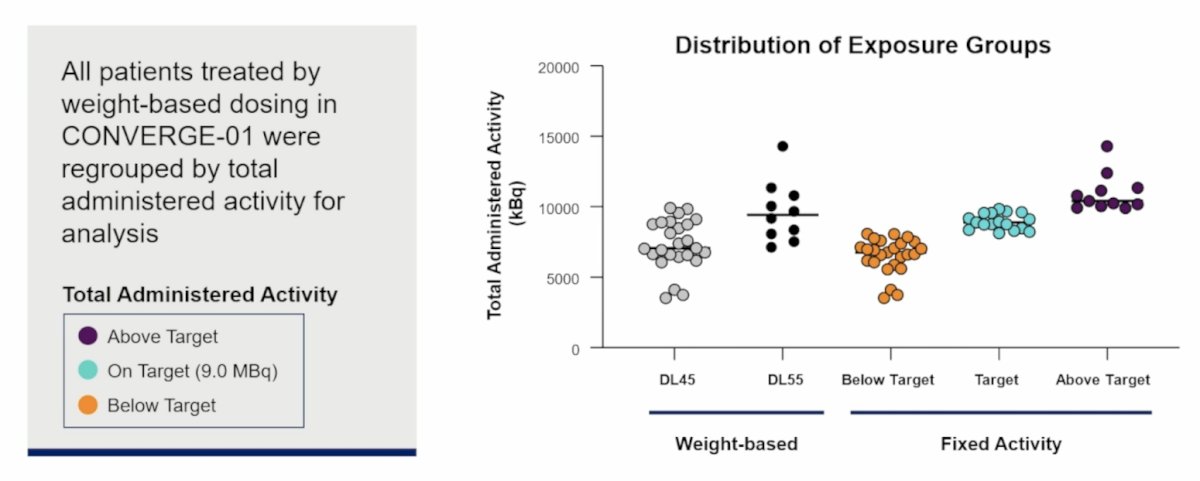
The primary endpoints were safety (CTCAE v5, all patients) and the proportion of patients with a decline in PSA of 50% or greater (PSA50) at the recommended phase 2 dose. Secondary endpoints included biodistribution and pharmacokinetic profile, while exploratory endpoints were biochemical progression-free survival, radiographic progression-free survival, genomic and imaging biomarkers. Enrollment into the dose-escalation and initial expansion cohorts of part 3 was conducted between August 2024 and December 2025. All patients treated by weight-based dosing in CONVERGE-01 were regrouped by total administered activity for the analysis:
For the data presented at ASCO 2026, there were 35 patients included, with a median age of 72 years (range: 58-83), a median PSA of 40.12 ng/dL (range: 4.16-1,910), and a median of 6 (range: 2-6) cycles of prior 177Lu-PSMA. Overall, 48.6% of patients had a history of xerostomia:

Dose escalation was completed without dose-limiting toxicities in all evaluable patients (n = 3 at DL45, n = 6 at DL55). The most common treatment-emergent adverse events were hematologic, digestive, and constitutional events. Grade 3+ treatment emergent adverse events were clinically manageable and generally transient; no treatment emergent adverse events led to treatment discontinuation. All high grade anemia was grade 3, but none were transfusion dependent. The 10 most common treatment-emergent adverse events are highlighted in the following figure:

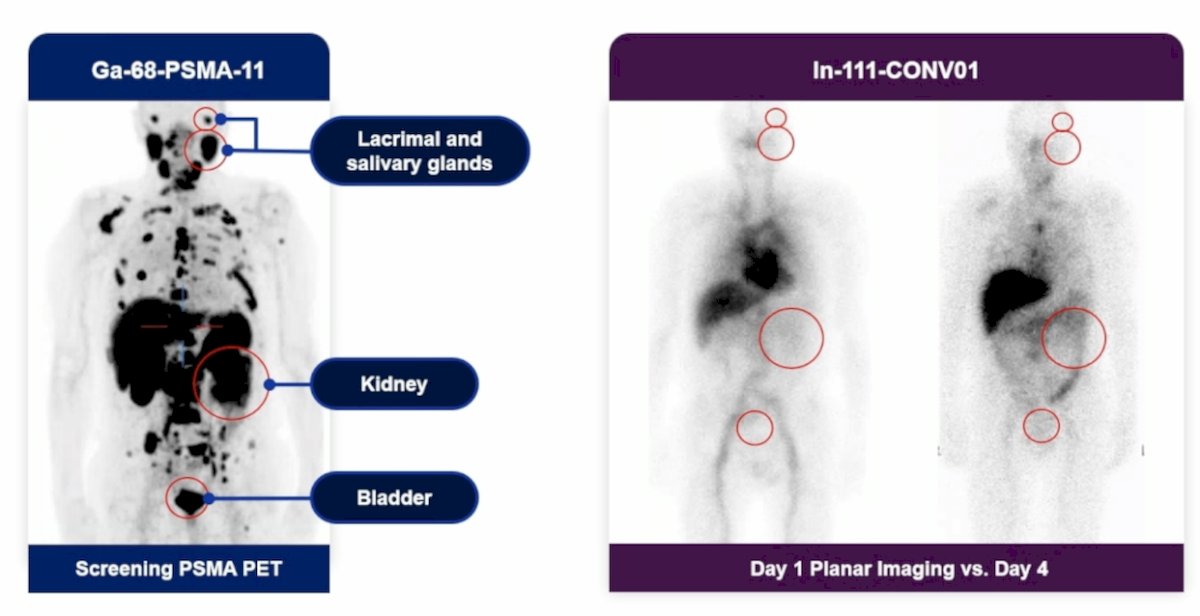
Of note, Dr. Morris emphasized that CONV01-α is not visualized in the salivary glands or the urinary system:
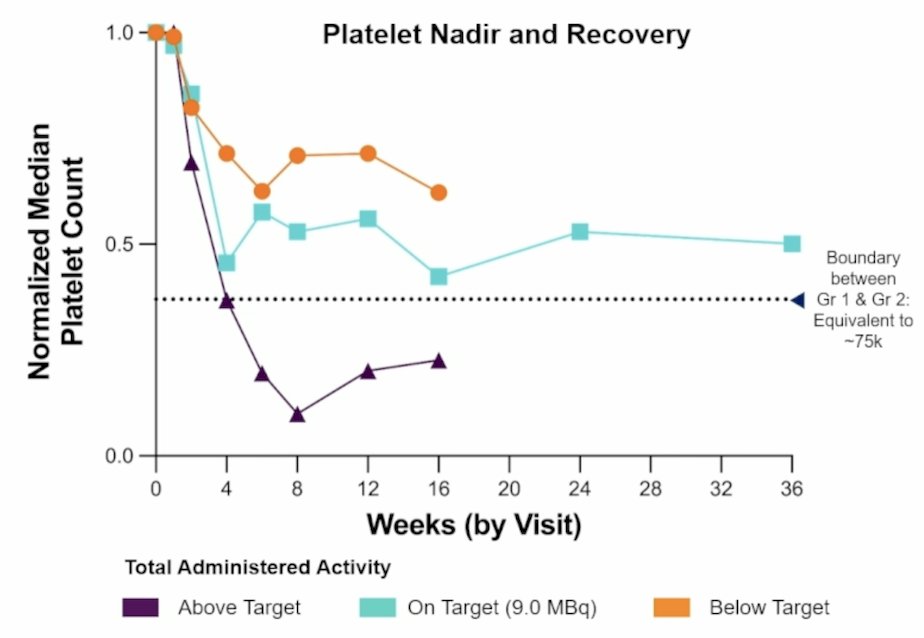
Thrombocytopenia was predictable, dose-related, and clinically manageable. Across the exposure groups, the populations experienced an early nadir, evidence of recovery, little evidence of clinical risk, and support for the target dose range:
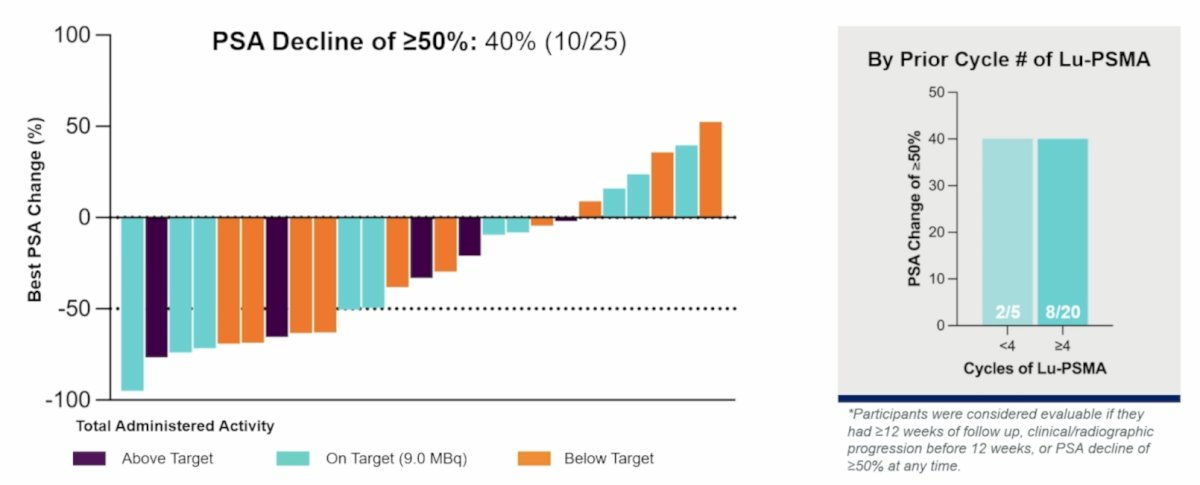
CONV01-α demonstrated promising activity in 177Lu-PSMA-617 exposed patients, with a PSA50 rate of 40%. By prior cycle number of 177Lu-PSMA-617, PSA50 rates were higher for those receiving >= 4 cycles:
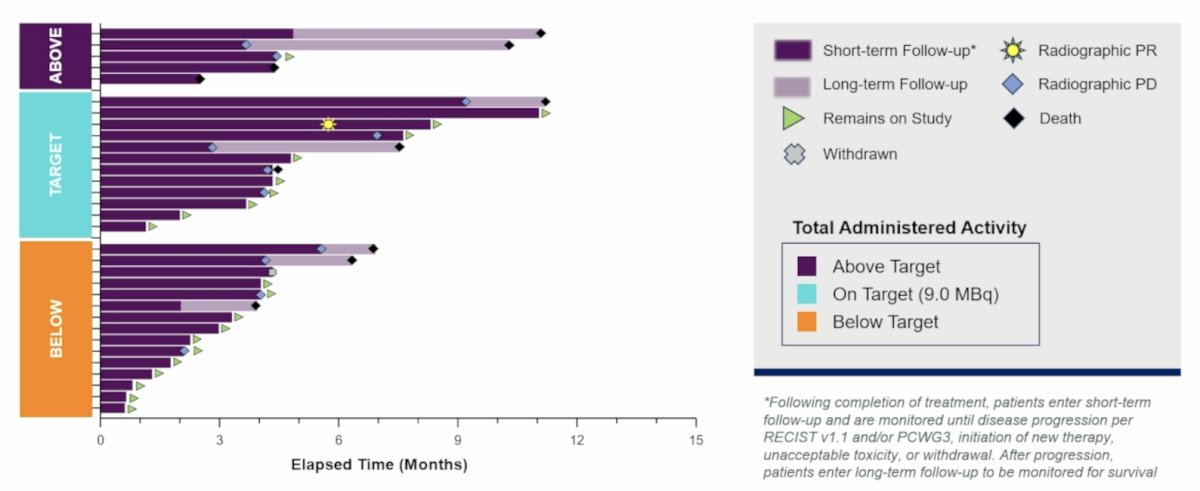
PSA50 rates were similar across dose groups, and the target dose group demonstrated greater durability:
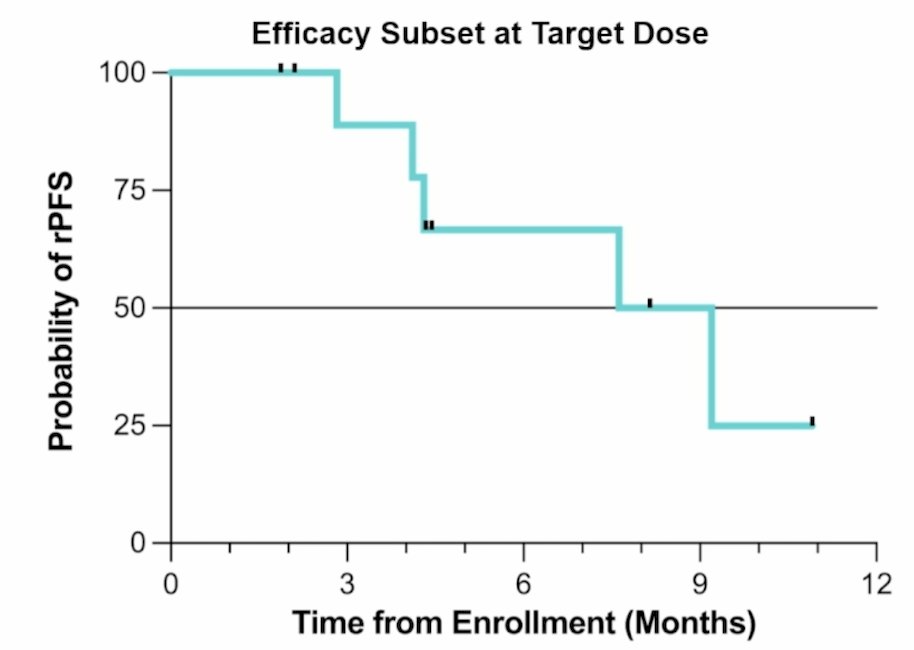
Preliminary radiographic progression-free survival supports clinical benefit in a high-unmet-need population. The median radiographic progression-free survival was 8.41 months (95% CI 2.83 – not reached) among 11 participants in the target dose range (9.0 MBq):
Dr. Morris concluded his presentation discussing CONVERGE-01 part 3, assessing CONV01-α in 177Lu-PSMA-617 pretreated mCRPC, with the following take-home points:
- CONV01-α is safe for patients with prior exposure to 177Lu-PSMA-617 radioligand therapy
- Hematologic toxicity was clinically manageable, and no nephrotoxicity or high-grade xerostomia
- CONV01-α has promising activity and durability in patients previously treated with 177Lu-PSMA-617
Presented by: Michael J. Morris, MD, Prostate Cancer Section Head, GU Oncology, Steven A. Greenberg Chair in Prostate Cancer Research, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Tagawa ST, Thomas C, Sartor AO, et al. Prostate-specific membrane antigen-targeting alpha emitter via antibody delivery for metastatic castration-resistant prostate cancer: A phase I dose-escalation study of 225Ac-J591. J Clin Oncol. 2024 Mar 1;842-851.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.