(UroToday.com) The 2026 ASCO annual meeting featured a radioligand innovation in prostate cancer session and a presentation by Dr. Pedro Barata discussing the preliminary results from part 1 of the phase 3 ProstACT Global study assessing the safety and dosimetry of 177Lu-rosopatamab tetraxetan (TLX591-Tx) + standard of care in patients with metastatic castration resistant prostate cancer (mCRPC). TLX591-Tx is a radiotherapeutic antibody to target PSMA, which was designed to address the following practical and biological considerations in mCRPC treatment:
- Safety and tolerability profile: low radiation to salivary glands and kidney, as well as transient and manageable hematological events
- Internationalization and retention: tumor payload and potential to maximize on-target effects
- Supply, access, and radiation protection: relatively lower administered activity
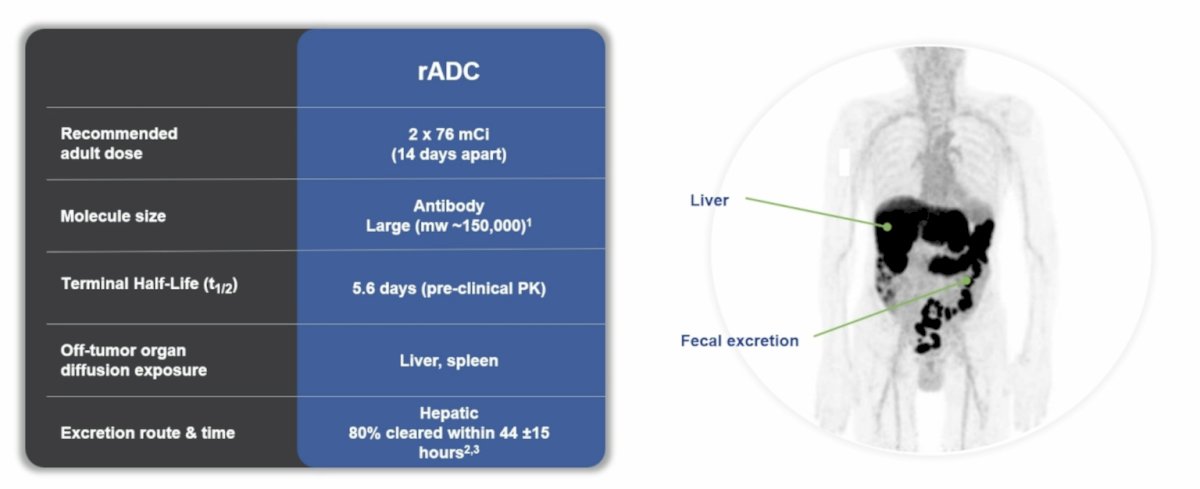
With regards to radioligand antibody drug conjugate pharmacokinetic and biodistribution, the recommended adult dose is 2 x 76 mCi (14 days apart), the molecule is large (mw ~150,000), the half life is 5.6 days (based on the preclinical pharmacokinetics), the off tumor organ diffusion exposure affects the liver and spleen, and the excretion route is hepatic (with 80% cleared within 44 +/- 15 hours):
ProstACT Global is a phase 3 study of TLX591-Tx + standard of care for patients with mCRPC. At ASCO 2026, Dr. Barata and colleagues presented the preliminary safety, dosimetry, and pharmacokinetics results from part 1 (lead-in).
Eligible patients for ProstACT Global had PSMA-positive mCRPC (confirmed on 68Ga-PSMA-11 PET/CT) with disease progression on ≥12 weeks of prior therapy on their first androgen receptor pathway inhibitor in metastatic castration sensitive prostate cancer (mCSPC), non-mCRPC, or mCRPC setting. Patients may have received docetaxel in the mCSPC setting if ≥6 months prior. Patients received two single IV injections of TLX591-Tx (76 mCi each), 14 days apart, with assigned standard of care: Cohort 1: + abiraterone; Cohort 2: + enzalutamide; Cohort 3: followed by docetaxel (planned for n = 10 each):
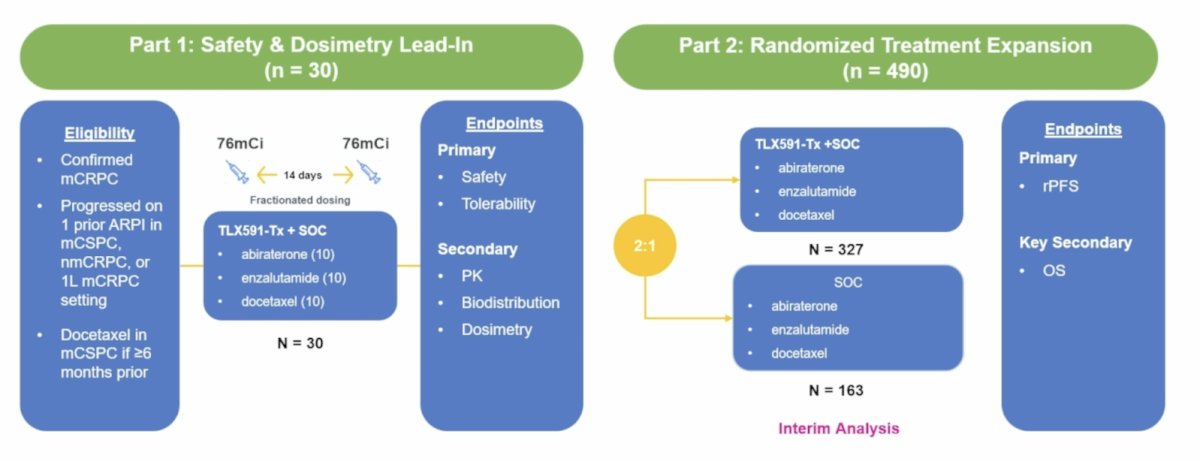
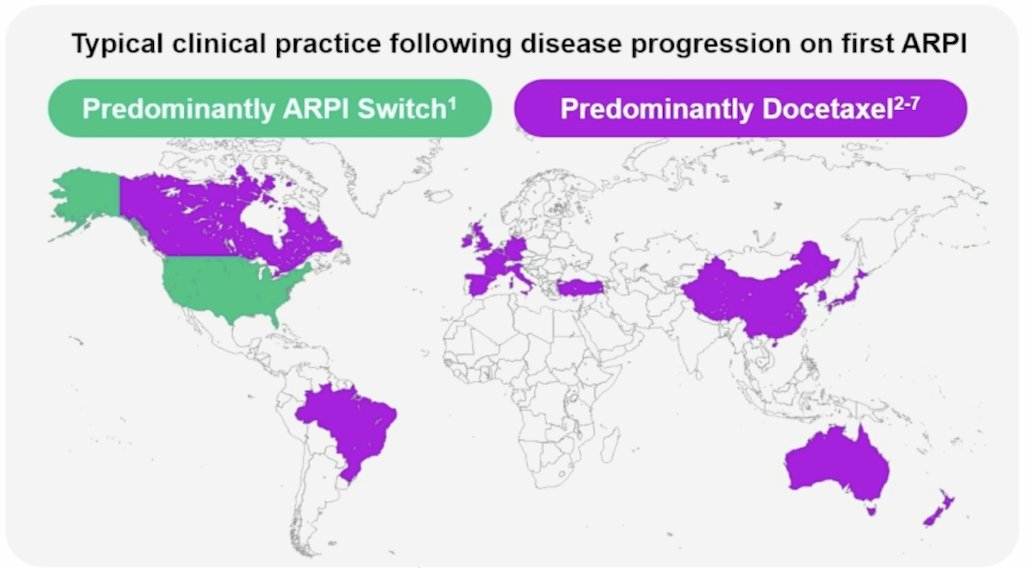
Patients were monitored for treatment-emergent adverse events (onset on or after initiation of study treatment). Patients underwent serial SPECT/CT imaging after TLX591-Tx administration (4, 24, 96, 168, 360 hours) for dosimetry and blood sampling for pharmacokinetics. The co-primary endpoints were safety and dosimetry of TLX591-Tx + standard of care. Analyses were preplanned, descriptive, and overseen by the IDMC. No formal statistics were performed. Dosimetry and biodistribution were evaluated using observed values without formal hypothesis testing. Of note, ProstACT Global was designed to accommodate regional treatment practices following progression on first ARPI, reflecting global clinical practice:
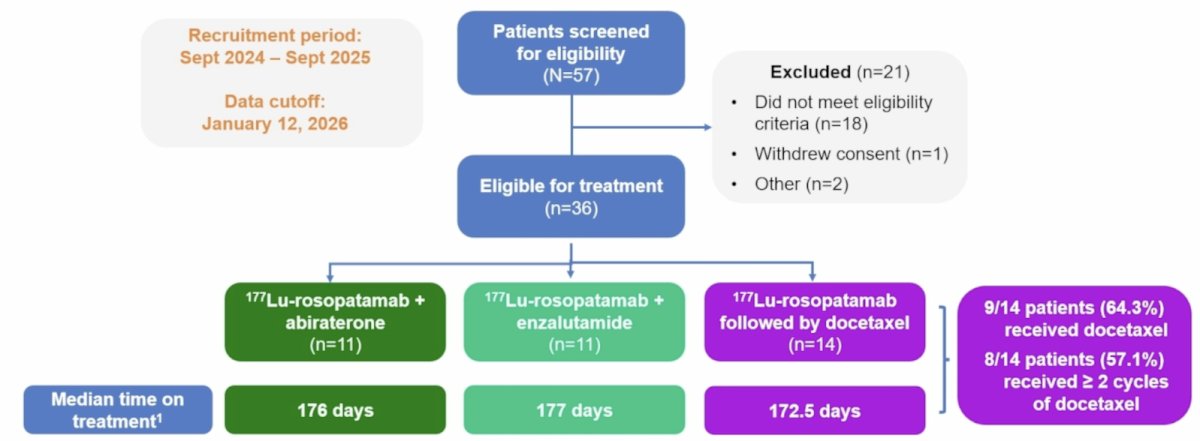
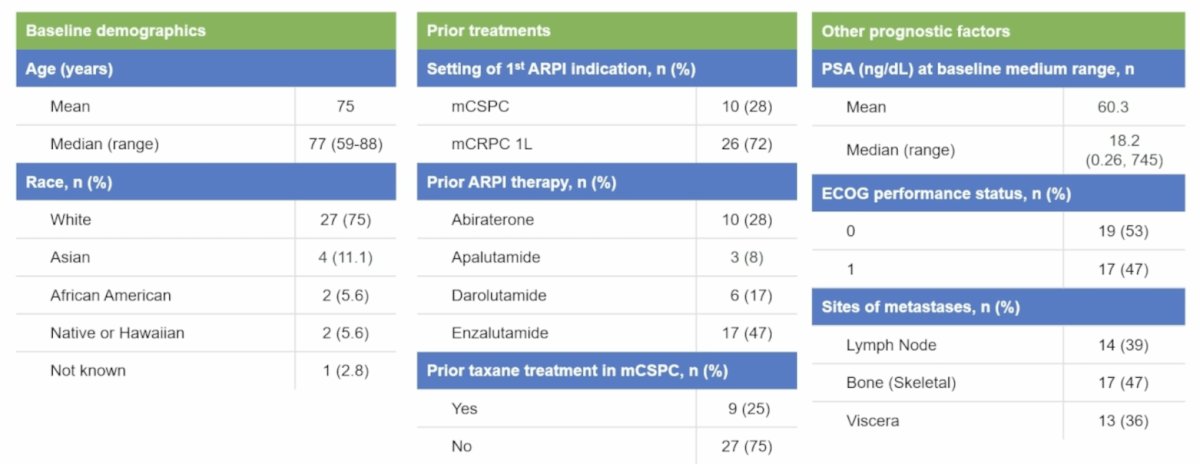
Data from 36 patients (baseline median PSA: 18.18 ng/mL) who received any study treatment were included (Cohorts 1, 2, 3: n = 11, 11, 14, respectively):
Overall, 55.6% patients had Gleason score 8-10 disease, 72% patients were evaluated for second-line mCRPC treatment, and 25% patients had previous taxane exposure:
No new safety signals were identified, and treatment-emergent adverse events were predominantly transient and manageable hematologic events. Hematologic treatment emergent adverse events included thrombocytopenia (any grade 77.8%; grade ≥3 44.4%), neutropenia (any grade 63.9%; grade ≥3 47.2%), and lymphopenia (any grade 55.6%; grade ≥3 41.7%). Non-hematologic treatment emergent adverse events were predominantly grade ≤2 fatigue (19 events, 53%), which was the most common, and only 9 (25%) xerostomia events were reported (all grade 1). No grade 5 treatment-related treatment emergent adverse events reported:
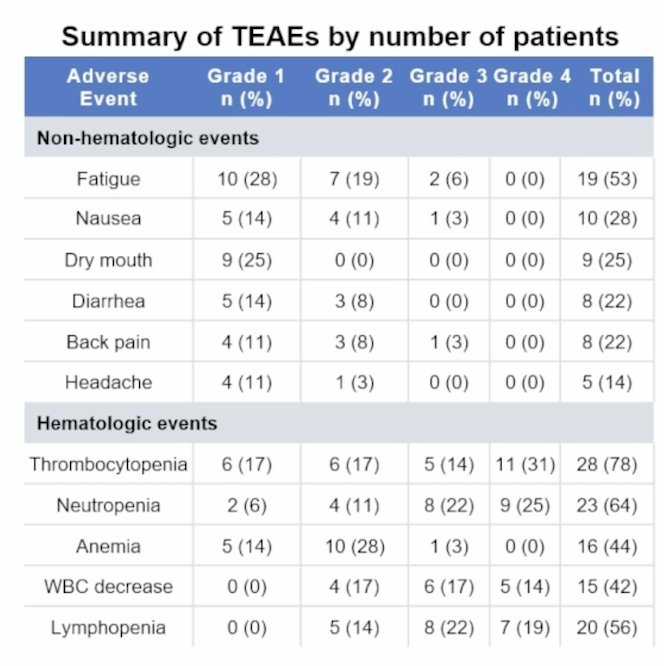
Specific to thrombocytopenia, the events were transient and consistent across the cohorts:
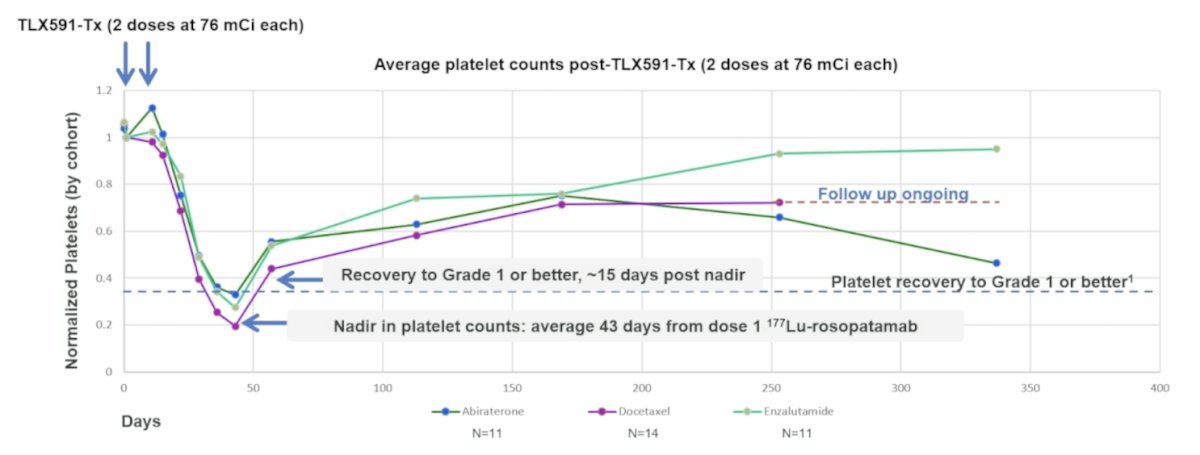
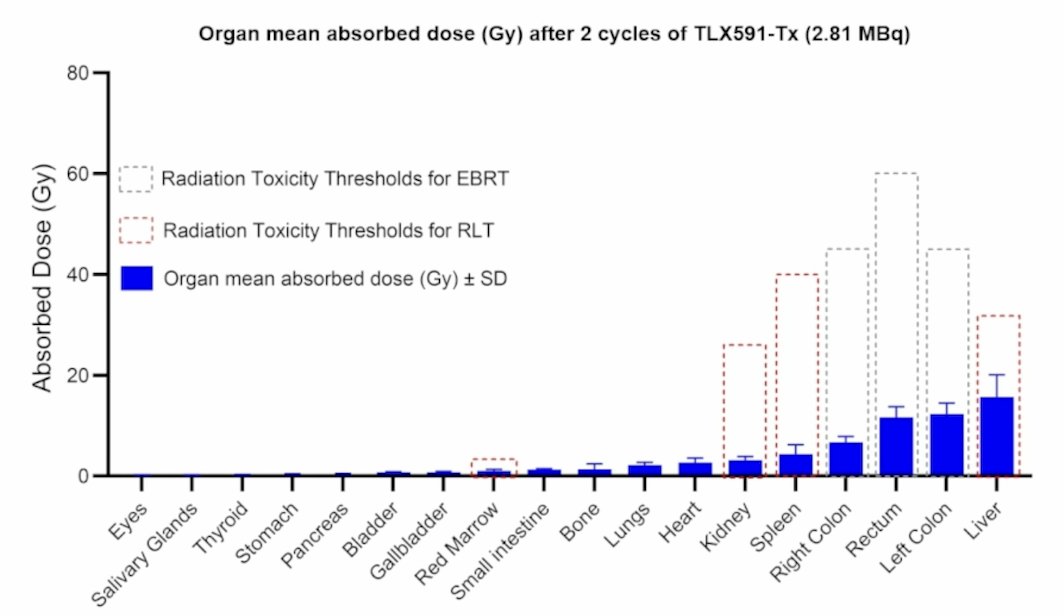
In terms of hematologic supportive interventions, there were only 5.6% of patients who had a red blood cell transfusion, 13.9% had a platelet transfusion, and 8.3% had G-CSF support. Blood activity concentration over time demonstrated bi-exponential clearance kinetics. Liver received the highest absorbed radiation (range, 1.62-5.08 mGy/MBq), with lower doses received by kidneys (0.336-0.961 mGy/MBq) and salivary glands (0.001-0.104 mGy/MBq). Lesion activity concentrations were higher than in normal tissues and detectable at the last imaging time point (15 days):
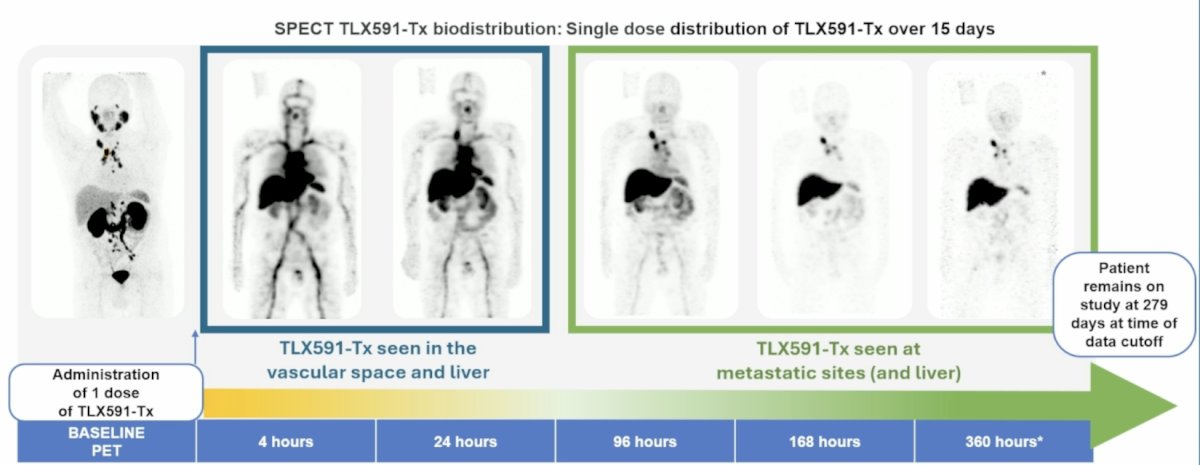
The first case presented by Dr. Barata was of a 64-year-old patient with metastatic disease in the lymph nodes treated with TLX591-Tx + abiraterone. He had a baseline PET and was subsequently treated with 1 dose of TLX591-Tx, which was seen in the vascular space and liver on SPECT at 4 hours and 24 hours, followed by TLX591-Tx seen at the metastatic sites and liver at 96 hours, 168 hours, and 360 hours. The patient remains on study at 279 days at the time of data cut-off:
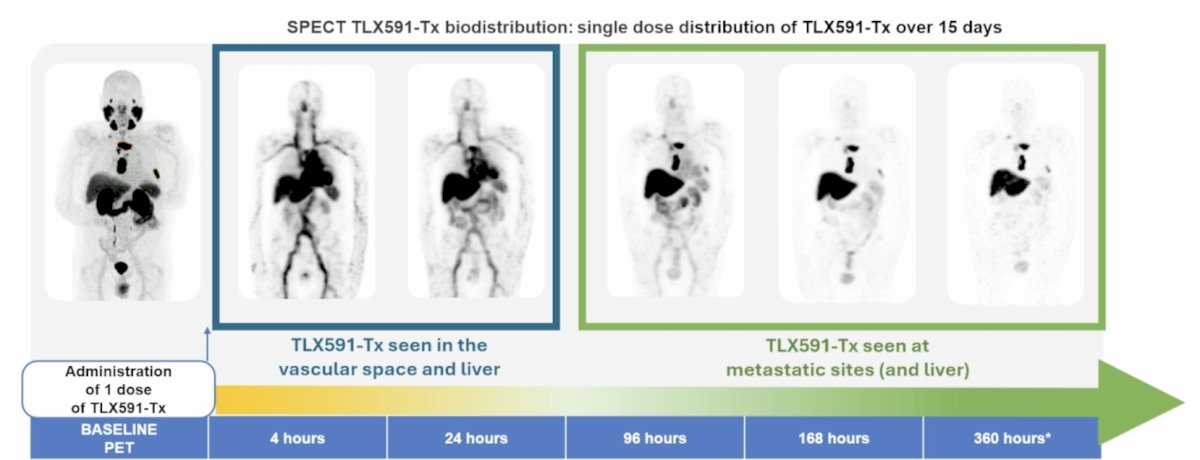
The second case was an 83-year-old patient with bone metastatic disease treated with TLX591-Tx and sequenced with docetaxel. Similarly, TLX591-Tx, which was seen in the vascular space and liver on SPECT at 4 hours and 24 hours, followed by TLX591-Tx seen at the metastatic sites and liver at 96 hours, 168 hours, and 360 hours:
Dr. Barata concluded his presentation discussing the preliminary results from part 1 of the phase 3 ProstACT Global study with the following take-home points:
- At the data cut-off of January 2026, 32 patients remain alive, and 26 patients are continuing in the study
- The observed safety and tolerability profile across TLX591-Tx + standard of care combination cohorts includes:
- Relatively low salivary gland and kidney radiation exposure observed in dosimetry analyses
- Sustained tumor-associated imaging signal through day 15, imaging shows prolonged tumor retention
- Treatment compliance and integration with the standard of care are feasible with a 2-dose regimen
- Supports the feasibility of integrating TLX591 with global standards of care, and the expansion phase is ongoing (NCT06520345)
Presented by: Pedro C. Barata, MD, MSc, FACP, Miggo Family Chair in Cancer Research, Co-Leader Genitourinary (GU) Disease Team, Director of GU Medical Oncology Research Program, University Hospitals Seidman Cancer Center, Associate Professor of Medicine, Case Western Reserve University, Case Comprehensive Cancer Center, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026