(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Rapid Oral Abstracts Session. Dr. Andrew J. Armstrong presented abstract 5016: Phase 2 multicenter trial of chemoimmunotherapy for patients with neuroendocrine or aggressive variant metastatic prostate cancer (CHAMP).
Dr. Armstrong began by highlighting the poor prognosis associated with neuroendocrine prostate cancer (NEPC) and aggressive-variant prostate cancer (AVPC), with median survival often less than one year.1 While platinum-doublet chemotherapy remains the standard of care, responses are typically short-lived, with historical 6-month radiographic PFS rates of approximately 55%.2
He further noted emerging evidence supporting immunotherapy-based combinations in this disease space. In the phase 2 C3NIRA study, the addition of cetrelimab (anti–PD-1) to cabazitaxel-carboplatin followed by niraparib maintenance improved both PFS and OS in men with AVPC.3 These findings, along with data from the CheckMate-9LA trial in NSCLC, provided the rationale for evaluating the CHAMP regimen, combining cabazitaxel-carboplatin with ipilimumab and nivolumab, with the hypothesis that this strategy could improve outcomes over chemotherapy alone while maintaining acceptable toxicity
The phase 2 CHAMP trial was designed as a two-stage, single-arm prospective multicenter study evaluating cabazitaxel-carboplatin combined with nivolumab and ipilimumab in patients with neuroendocrine prostate cancer (NEPC) or aggressive-variant prostate cancer (AVPC). Eligible patients were required to have histologic evidence of small cell/NEPC or clinical or molecular features consistent with AVPC, prior ARPI exposure, no prior cabazitaxel, and a Karnofsky Performance Status ≥70.
Patients received carboplatin, cabazitaxel, nivolumab, and ipilimumab alongside ongoing ADT for up to 10 cycles, followed by maintenance nivolumab plus ipilimumab until progression or unacceptable toxicity. The primary endpoint was 6-month radiographic PFS by immune-modified RECIST 1.1/PCWG3 criteria. Overall, 43 patients were enrolled across stages I and II of the study.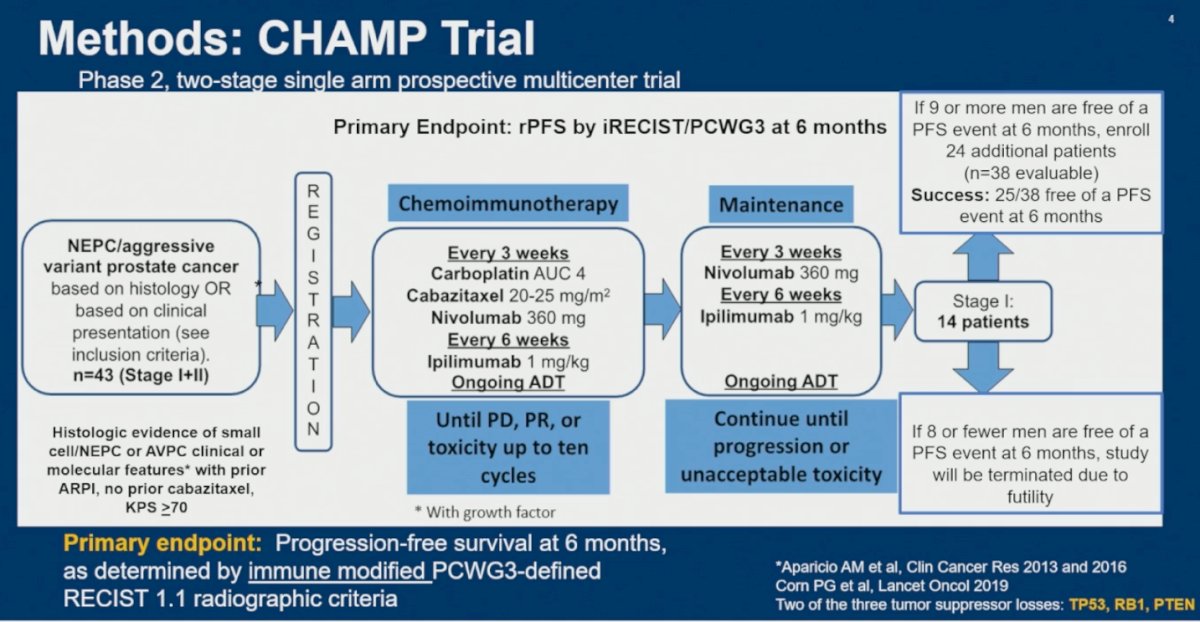
The study population was enriched for AVPC and NEPC features, with 70% classified as AVPC and 30% as NEPC. Visceral metastatic involvement was common, including liver metastases in 58% and lung metastases in 33% of patients. Median baseline PSA was notably low at 2 ng/mL, consistent with the androgen-indifferent biology typically observed in AVPC/NEPC, while 88% had elevated AVPC-associated serum biomarkers, including CEA, chromogranin A, or LDH. Patients were heavily pretreated, with 93% previously exposed to ARPIs, 78% having received prior chemotherapy, and 15% prior platinum-based chemotherapy. Molecular profiling demonstrated frequent TP53, RB1, and PTEN alterations, including overlapping alterations across these lineage-plasticity drivers. Notably, only one patient had MSI-high disease, and the median tumor mutational burden was low at 3 mutations/Mb.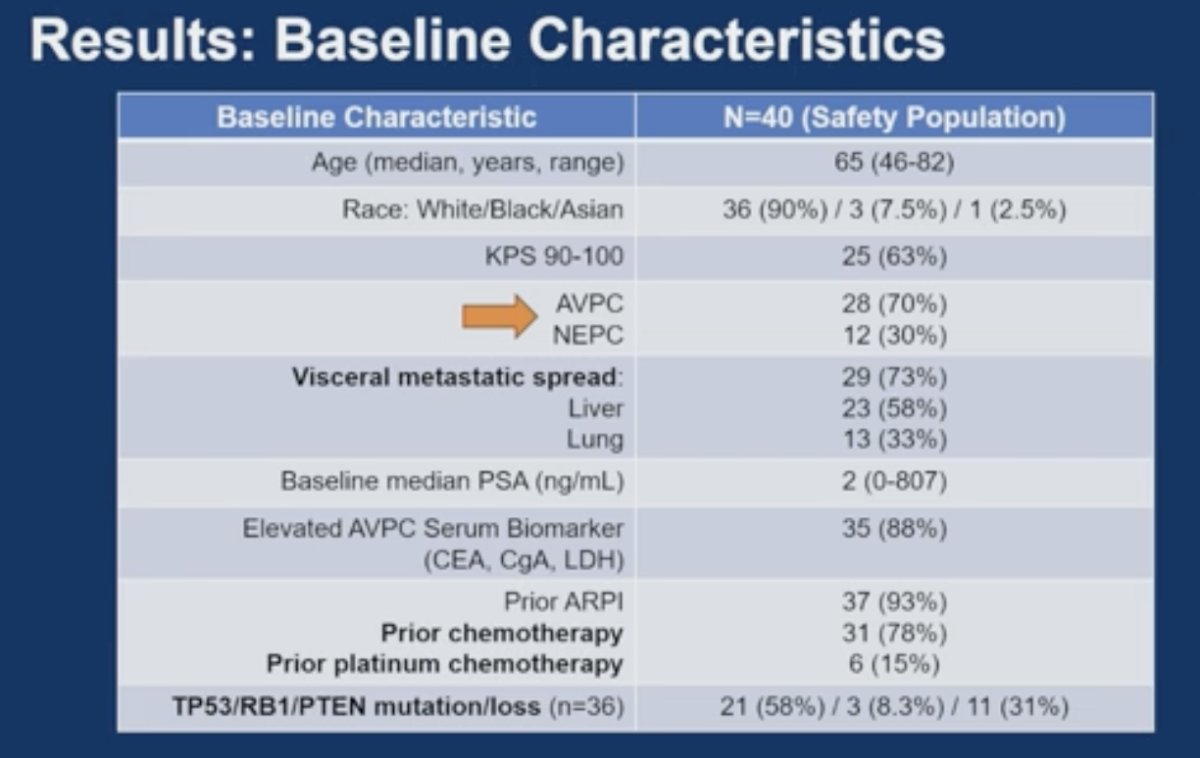
The CHAMP regimen met its primary endpoint, with a 6-month immune-modified rPFS rate of 74% (28/38 patients; 90% CI 63–100%), significantly exceeding the historical control benchmark of 55% (p=0.013). With a median follow-up of 18 months, median immune-modified rPFS was 12 months (95% CI 9.1–14), supporting meaningful clinical activity of cabazitaxel-carboplatin combined with nivolumab and ipilimumab in this AVPC/NEPC population.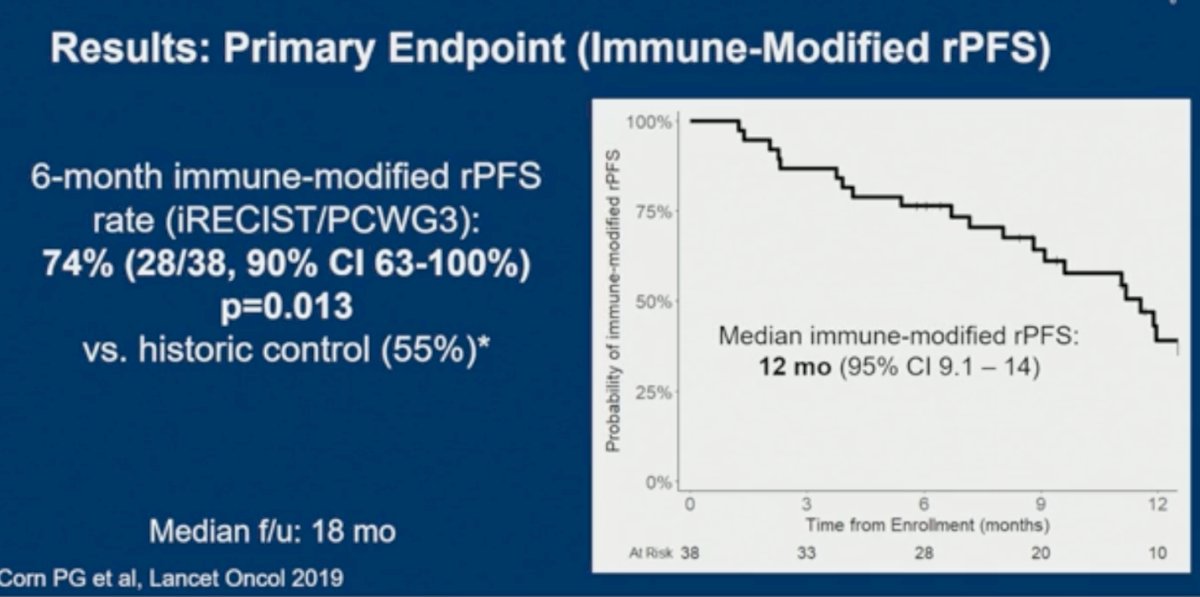
Secondary endpoint analyses showed a median RECIST-based rPFS of 6.1 months, while median OS reached 12 months, which falls within the historical range reported with cabazitaxel plus carboplatin alone in AVPC (9.9–17.4 months). Importantly, despite RECIST progression in many patients, there was a tail on the OS curve, with 23% of patients alive at 2 years, including 14% with AVPC and 36% with NEPC. The ORR by iRECIST was 37% (95% CI 22–54%), with a median duration of response of 9.3 months.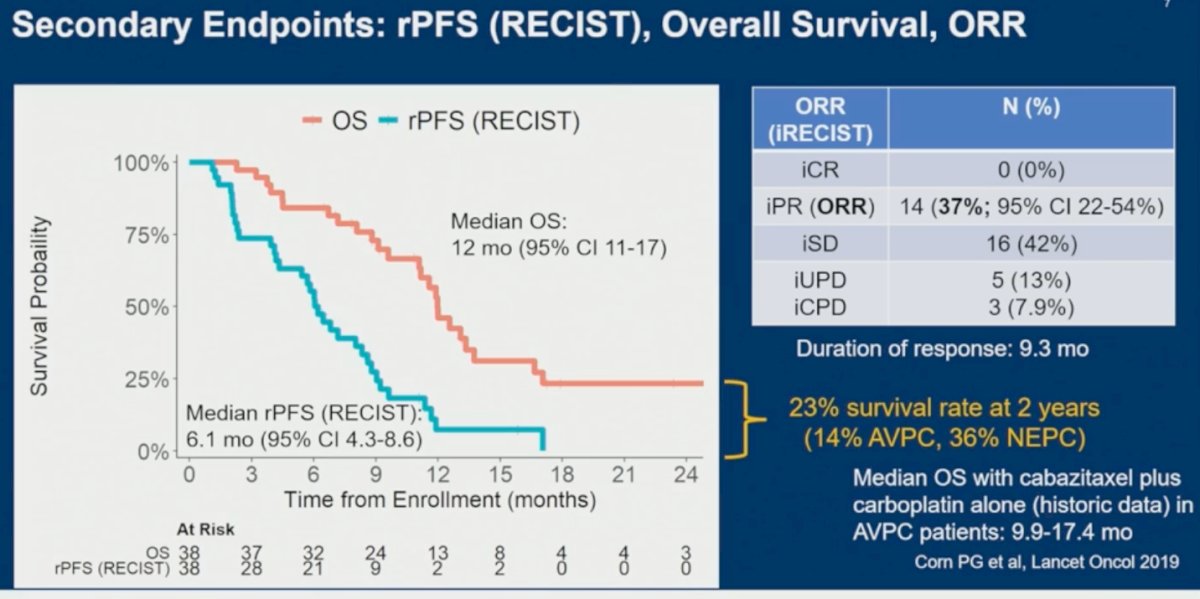
Swimmer plot analyses demonstrated durable benefit in a subset of patients, with two patients remaining disease-free and off therapy beyond 30 months. Several patients also experienced initial unconfirmed progression followed by stable disease or partial response by iRECIST, supporting the potential for delayed immunotherapy responses in this population. Interestingly, RB1 loss appeared to be associated with shorter swim lanes and less durable clinical benefit, suggesting a potential relationship between lineage-plasticity alterations and resistance to therapy.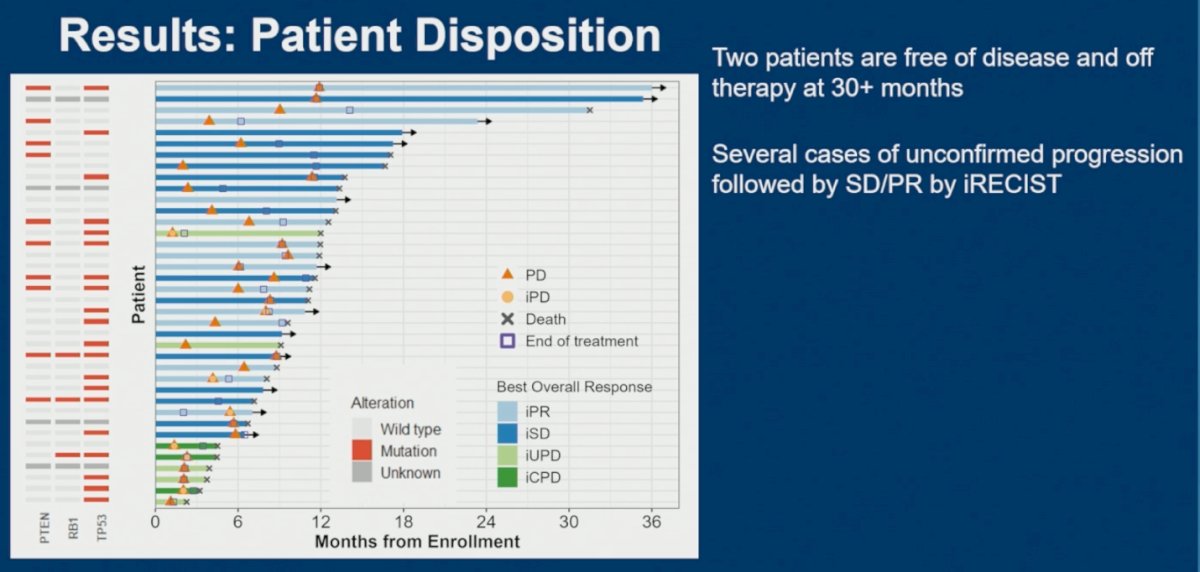
Lastly, the CHAMP regimen demonstrated a manageable safety profile, with most treatment-related adverse events being grade 1–2. The most common toxicities included anemia, nausea, fatigue, diarrhea, thrombocytopenia, and hypomagnesemia. Febrile neutropenia occurred in 10% of patients, while grade 3 and 4 toxicities were observed in 16% and 3% of patients, respectively. Importantly, there were no treatment-related grade 5 events or fatal toxicities. Immune-related adverse events were uncommon and included one case of grade 3 myositis and one case of grade 2 pneumonitis. Although severe adverse events such as sepsis, urinary tract infections, colitis, and acute kidney injury were reported, all treatment-related serious adverse events resolved, and none were fatal.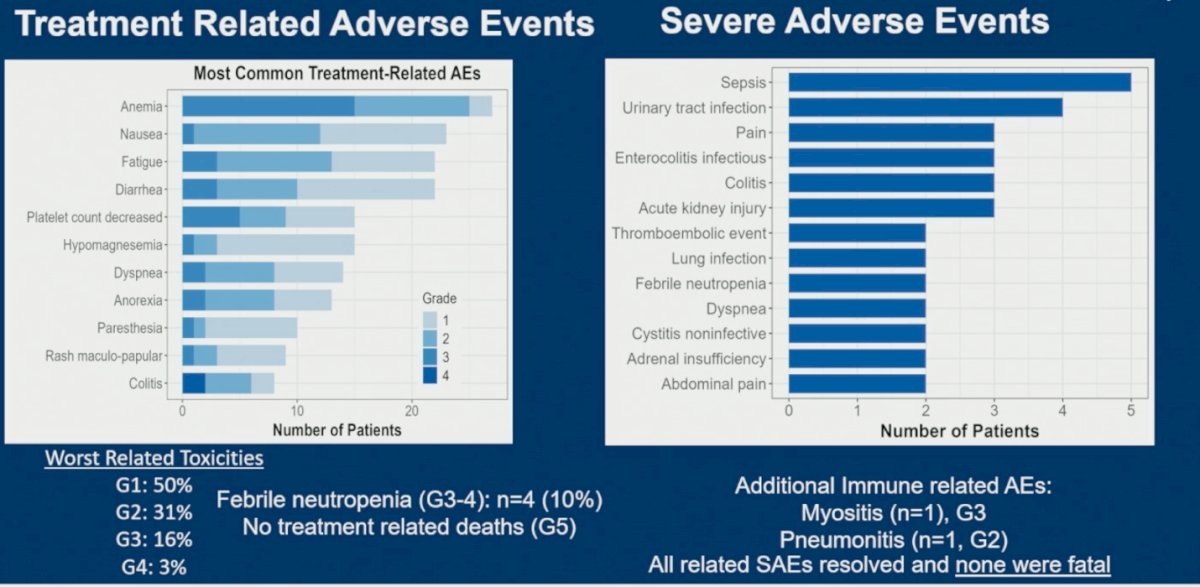
Dr. Armstrong wrapped up his presentation with the following key points:
- Chemoimmunotherapy with dual PD-1/CTLA-4 blockade combined with cabazitaxel/carboplatin was feasible and demonstrated acceptable toxicity in patients with NEPC/AVPC.
- The regimen improved the 6-month rPFS rate to 74% compared with the historical benchmark of 55% for platinum-doublet chemotherapy alone (p=0.013).
- Median immune-modified rPFS by iRECIST/PCWG3 criteria was 12 months.
- Durable clinical benefit was observed in a subset of patients, including a 23% survival rate at 2 years despite progression by conventional RECIST criteria.
- These findings support further investigation of chemoimmunotherapy strategies in NEPC/AVPC.
- Randomized controlled trials are needed to better define the overall risk-benefit profile of chemoimmunotherapy in this population, including its impact on progression, survival, quality of life, and long-term toxicity.
Presented by: Andrew Armstrong, MD, MSc, Medical Oncologist, Professor of Medicine, Surgery, Pharmacology and Cancer Biology, Duke Cancer Institute, Center for Prostate and Urologic Cancers, Durham, NC
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
- Aparicio AM, Harzstark AL, Corn PG, Wen S, Araujo JC, Tu SM, Pagliaro LC, Kim J, Millikan RE, Ryan C, Tannir NM, Zurita AJ, Mathew P, Arap W, Troncoso P, Thall PF, Logothetis CJ. Platinum-based chemotherapy for variant castrate-resistant prostate cancer. Clin Cancer Res. 2013 Jul 1;19(13):3621-30. doi: 10.1158/1078-0432.CCR-12-3791. Epub 2013 May 6. PMID: 23649003; PMCID: PMC3699964.
- Corn PG, Heath EI, Zurita A, Ramesh N, Xiao L, Sei E, Li-Ning-Tapia E, Tu SM, Subudhi SK, Wang J, Wang X, Efstathiou E, Thompson TC, Troncoso P, Navin N, Logothetis CJ, Aparicio AM. Cabazitaxel plus carboplatin for the treatment of men with metastatic castration-resistant prostate cancers: a randomised, open-label, phase 1-2 trial. Lancet Oncol. 2019 Oct;20(10):1432-1443. doi: 10.1016/S1470-2045(19)30408-5. Epub 2019 Sep 9. Erratum in: Lancet Oncol. 2020 Jan;21(1):e14. doi: 10.1016/S1470-2045(19)30754-5. PMID: 31515154; PMCID: PMC6858999.
- Ana Aparicio et al., C3NIRA: Randomized phase II study of carboplatin-cabazitaxel-cetrelimab (anti-PD-1) induction followed by niraparib +/- cetrelimab maintenance in men with aggressive variant prostate cancers (AVPC).. J Clin Oncol 43, 5008-5008(2025) DOI:10.1200/JCO.2025.43.16_suppl.5008