(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Rapid Oral Abstracts Session. Dr. Nancy P. Mendenhall presented Late Breaking abstract LBA5012: Early results of COMPPARE, a prospective comparison of outcomes with proton and photon radiation in prostate cancer.
Dr. Mendehall highlighted that proton therapy (PT) is a promising radiation modality that reduces radiation dose to non-targeted tissues and is broadly accepted in select disease sites, with recent Level I evidence demonstrating improved toxicity, quality of life, and survival outcomes in oropharyngeal cancer. However, less than 2% of prostate cancer patients receiving radiation undergo PT. Single institutions have reported toxicity, quality of life, and disease control outcomes with PT that appear comparable or superior to conventional intensity-modulated radiation therapy (IMRT), and modeling and normal tissue complication probability studies have demonstrated potential reductions in second malignancy risk. Despite these potential advantages, prospective comparative effectiveness data in prostate cancer remain lacking.
Dosimetric comparison demonstrated substantially lower radiation exposure to non-targeted tissues with proton therapy relative to conventional IMRT. Specifically, proton therapy reduced dose to normal tissues by approximately 50% compared with IMRT, with the dose distribution visualization illustrating minimal moderate-to-low dose exposure in surrounding tissues with PT versus more extensive dose exposure observed with conventional IMRT.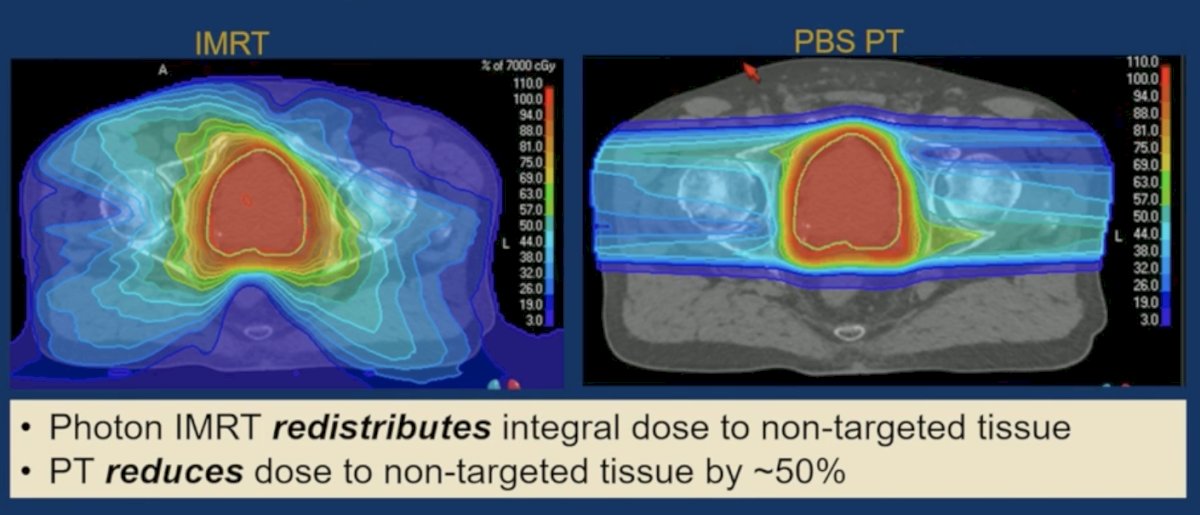
This knowledge gap led to the COMPPARE study, a prospective, pragmatic comparison of outcomes between proton therapy and photon radiation (IMRT) in patients with de novo prostate cancer, excluding very high-risk and metastatic disease. Funded by the Patient-Centered Outcomes Research Institute (PCORI), the study enrolled patients across 51 proton therapy and IMRT centers, with accrual occurring from July 2018 through October 2022. The eligible cohort comprised 1,500 proton therapy and 1,000 photon therapy patients.
Dr. Mendenhall reviewed the baseline characteristics of the study population presented in the table below. Notably, median patient age was 69 years, with 79.3% of patients identified as White and 16.8% as Black. Most patients had lower-risk disease features, including PSA <10 ng/mL in 74.1%, Gleason score 6–7 disease in 89.2%, and clinical T1/T2 disease in 98.4% of cases. Intermediate-risk disease comprised the majority of the cohort (74.4%), while 17.0% had high-risk disease. In addition, 74.5% of patients had an ACE comorbidity score ≥1, hypofractionation was used in 59.5% of patients, rectal spacers in 75%, and ADT in 50.6%.
Inverse probability of treatment weighting (IPTW) was performed to improve comparability between cohorts and reduce baseline imbalances. Age, race, insurance status, PSA, Gleason score, and patient prioritization variables were prespecified for propensity adjustment in the research plan. Following IPTW adjustment, the covariates demonstrated appropriate balance between cohorts, supporting the validity of subsequent comparative analyses.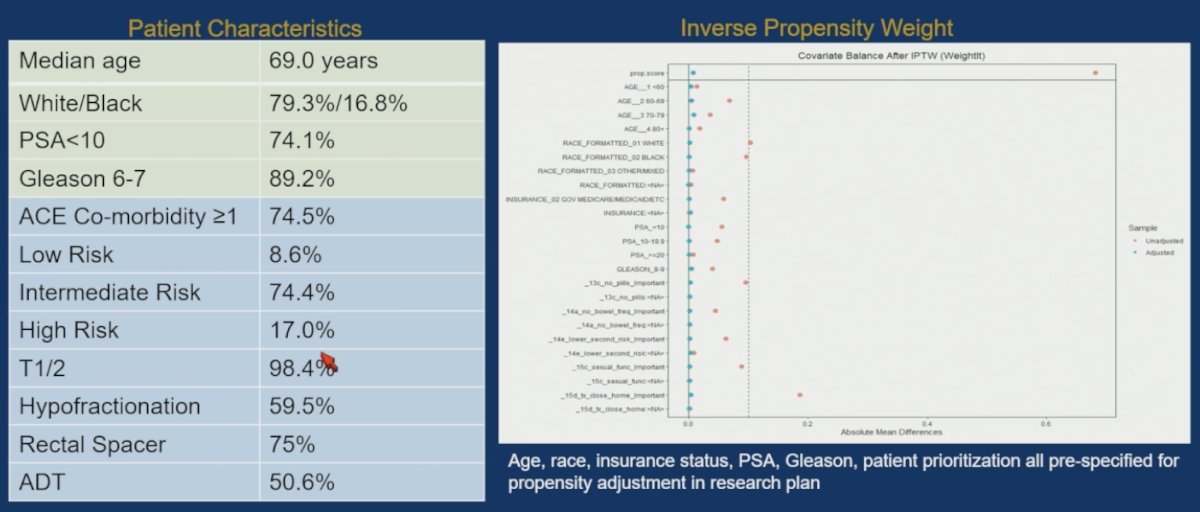
Hypothesized gastrointestinal toxicity rates with proton therapy were substantially higher than the actual observed rates. While the study anticipated clinically meaningful reductions in bowel urgency, bowel frequency, and grade ≥2 GI toxicity with PT compared with IMRT, the observed toxicity rates were low in both groups, and no statistically significant differences were identified. Likewise, freedom from disease progression at 3 years was excellent and nearly identical between cohorts (97.9% vs 98.0%; p=0.90).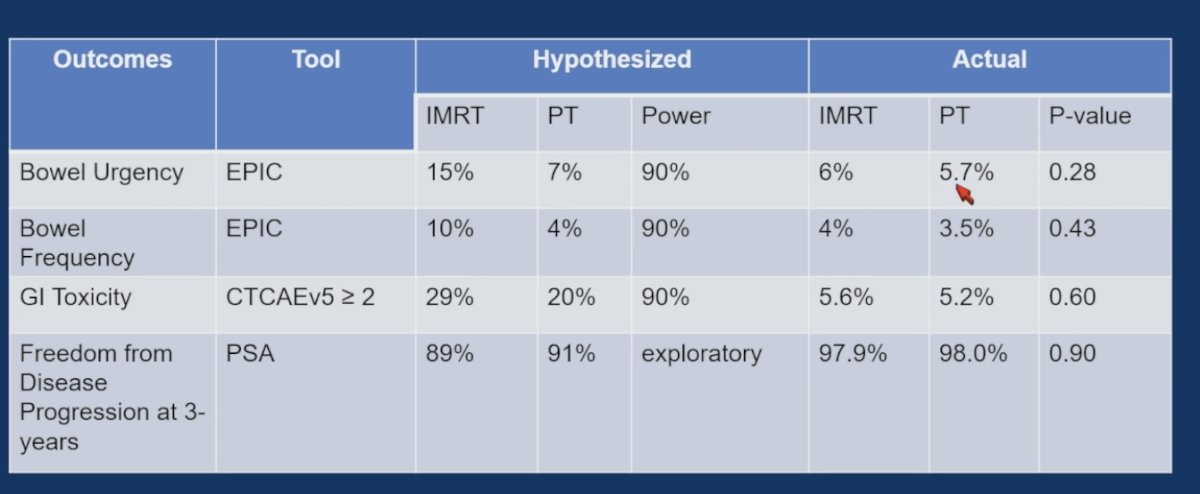
Lastly, the impact of rectal spacers could not be overlooked. The FDA approved the use of rectal spacers to reduce radiation injury to the rectum on April 1, 2015. The 2-year cumulative CTCAE V5 GI Grade 2+ toxicity was 4.4% IMRT group vs 4.7% in the PT group among patients who had a rectal spacer and 7.2% vs 8.7% amongst those who did not have a rectal spacer, and this was statistically significant.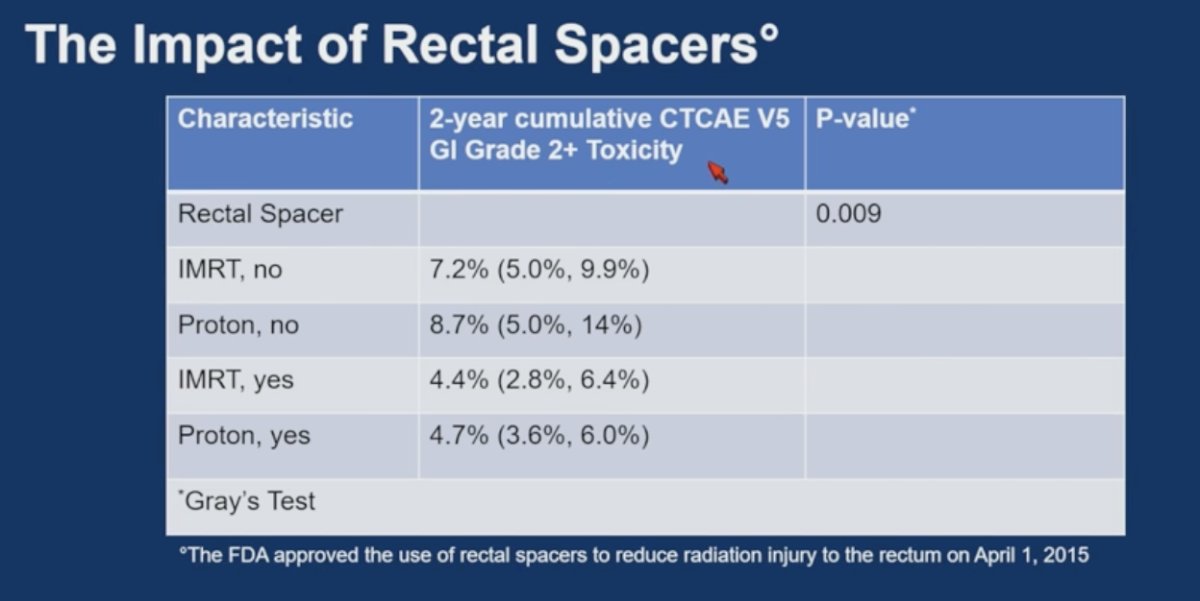
Dr. Mendenhall wrapped up her presentation with the following key takeaway points:
- The COMPPARE study demonstrated excellent early outcomes with both IMRT and proton therapy as treatment modalities for localized prostate cancer
- Radiation-induced rectal and bowel toxicity was significantly reduced in both treatment groups with the use of temporary rectal spacers
- No significant early differences were observed between IMRT and proton therapy with respect to patient-reported quality of life, toxicity outcomes, or freedom from PSA progression
- Based on these findings, both IMRT and proton therapy should be considered standard-of-care radiation options
- The study findings are broadly applicable to most patients with localized prostate cancer, excluding those with very high-risk or metastatic disease
- An important limitation is that assessment of long-term comparative outcomes, including disease control, late toxicity, and secondary malignancies, will require longer follow-up
Presented by: Nancy P. Mendenhall, MD, FACR, FASTRO, Radiation oncologist at the UF Health Proton Therapy Institute. Jacksonville, FL
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026