(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a prostate, testicular, and penile cancers poster session. Dr. Ugo De Giorgi presented a post hoc analysis from the phase 3 TALAPRO-2 trial evaluating the impact of baseline demographic characteristics on talazoparib (TALA) dose modifications and clinical outcomes among patients with metastatic castration-resistant prostate cancer (mCRPC) treated with talazoparib plus enzalutamide (ENZA).
As previously reported, TALAPRO-2 demonstrated significant improvements in radiographic progression-free survival (rPFS) with TALA + ENZA versus placebo (PBO) + ENZA in both the unselected population (HR 0.63, 95% CI 0.51–0.78; p<0.0001) and the homologous recombination repair (HRR)-deficient population (HR 0.45, 95% CI 0.33–0.61; p<0.0001).1 Final overall survival (OS) analyses also demonstrated statistically significant and clinically meaningful improvements with TALA + ENZA in both cohorts. Because anemia was the most common treatment-emergent adverse event (TEAE) and dose reductions were mandated for grade 3–4 hematologic toxicities, the investigators sought to determine whether baseline demographic characteristics influenced TALA dose reductions and whether these modifications affected treatment outcomes.
Patients in the TALA + ENZA arm received talazoparib 0.5 mg daily (0.35 mg daily in patients with moderate renal impairment) plus ENZA 160 mg daily. Dose reductions were permitted sequentially to 0.35, 0.25, and 0.1 mg daily. The primary endpoint of TALAPRO-2 was blinded independent central review (BICR)-assessed rPFS, with OS as a key alpha-protected secondary endpoint.
In the unselected cohort, 228/398 patients (57.3%) experienced at least one TALA dose reduction, including 216 due to adverse events. A total of 115 patients (28.9%) underwent one dose reduction, and 113 (28.4%) underwent multiple reductions. Median time to first dose reduction was 17.4 weeks. TALA interruptions and/or reductions due to grade 1–2 TEAEs occurred in 247 patients (62.1%), most commonly grade 1–2 anemia (46.7%). Notably, more patients without dose reductions discontinued treatment before week 16 compared with those who underwent dose reductions (20.0% versus 6.1%). Median duration of treatment with TALA was longer among patients who underwent dose reductions compared with those who did not (23.0 versus 15.2 months).
Similarly, in the HRR-deficient cohort, 111/198 patients (56.1%) experienced at least one TALA dose reduction, including 108 due to adverse events. Median time to first dose reduction was 15.7 weeks. TALA interruptions and/or reductions due to grade 1–2 TEAEs occurred in 59.6% of patients, again primarily due to grade 1–2 anemia (45.5%). Early treatment discontinuation prior to week 16 occurred less frequently among patients who underwent dose reductions than among those who did not (2.7% versus 13.8%). Median duration of treatment was similar between patients with and without dose reductions (20.3 versus 20.8 months).
Table 1 summarizes reasons for treatment discontinuation among patients with treatment duration <16 weeks. Across both cohorts, adverse events represented the most common reason for early discontinuation. In the unselected population, adverse-event-related discontinuation occurred in 12.9% of patients without dose reductions compared with 3.5% among those with dose reductions. Similar findings were observed in the HRR-deficient cohort (4.6% versus 2.7%, respectively).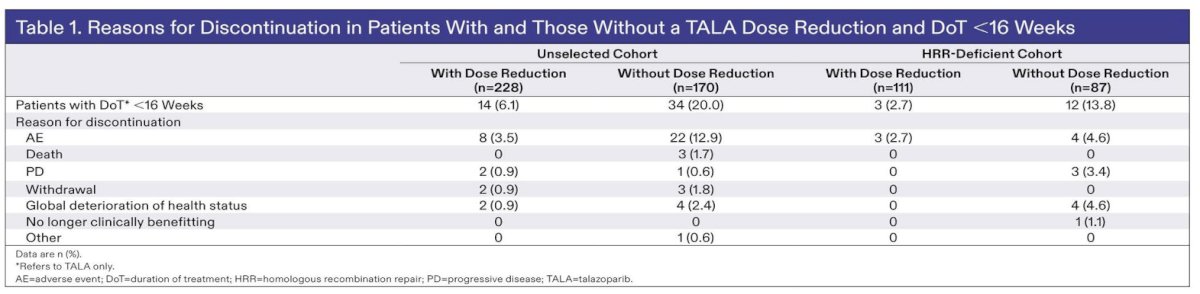
Table 2 evaluated baseline demographic characteristics associated with TALA dose reductions. Across both the unselected and HRR-deficient cohorts, patients who required dose reductions were generally older, more likely to be of Asian ethnicity, had lower body weight, and were more likely to have mild renal impairment compared with patients who did not require dose reductions. Baseline anemia was also more common among patients who subsequently underwent dose reductions. In the unselected cohort, baseline anemia was present in 53.9% of patients with dose reductions versus 42.4% without; corresponding rates in the HRR-deficient cohort were 60.4% and 49.4%, respectively.
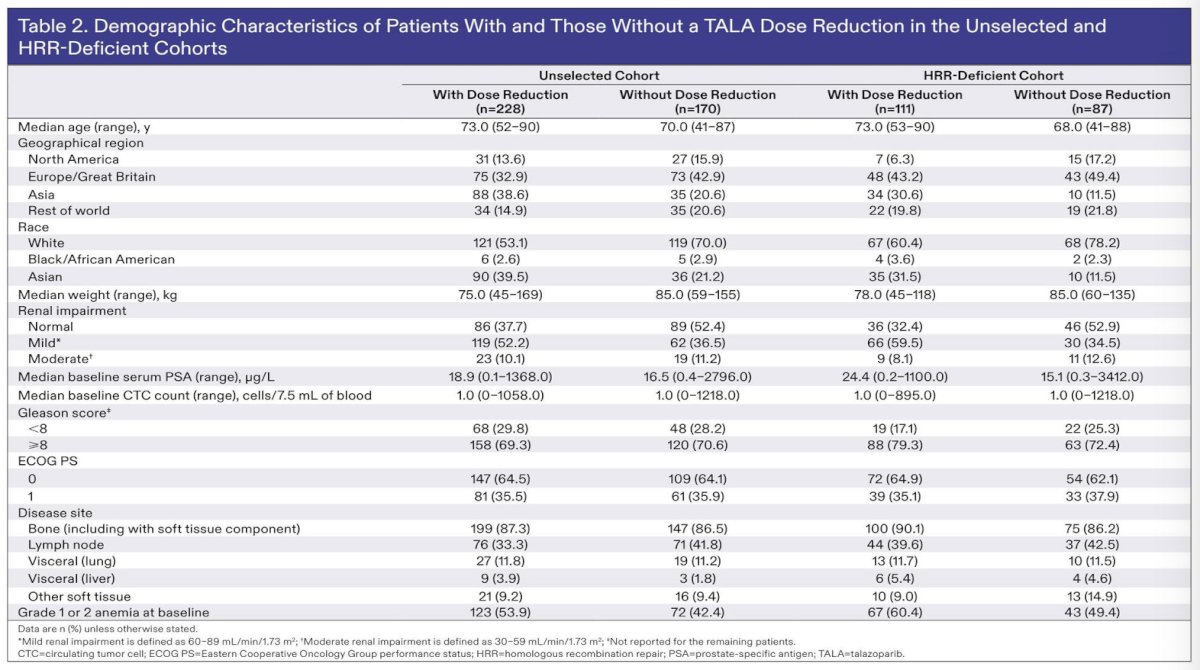
Figure 1 demonstrates BICR-assessed rPFS according to TALA dose reduction status. In the unselected cohort, median rPFS was 33.1 months (95% CI 27.4–41.4) among patients with dose reductions and 33.0 months (95% CI 22.3–41.4) among those without dose reductions (HR 0.94, 95% CI 0.70–1.25; p=0.66). Similarly, in the HRR-deficient cohort, median rPFS was 33.1 months (95% CI 24.3–38.5) among patients with dose reductions and 30.2 months (95% CI 18.1–46.7) among those without dose reductions (HR 0.96, 95% CI 0.64–1.44; p=0.84). These findings indicate no clinically meaningful difference in rPFS according to dose reduction status.
OS findings were likewise consistent across dose reduction groups. In the unselected population, median OS was 46.9 months among patients with dose reductions versus 45.1 months among those without (HR 0.90, 95% CI 0.68–1.20). In the HRR-deficient cohort, median OS was 41.9 months versus 48.4 months, respectively (HR 0.98, 95% CI 0.64–1.49), again demonstrating no clinically meaningful differences.
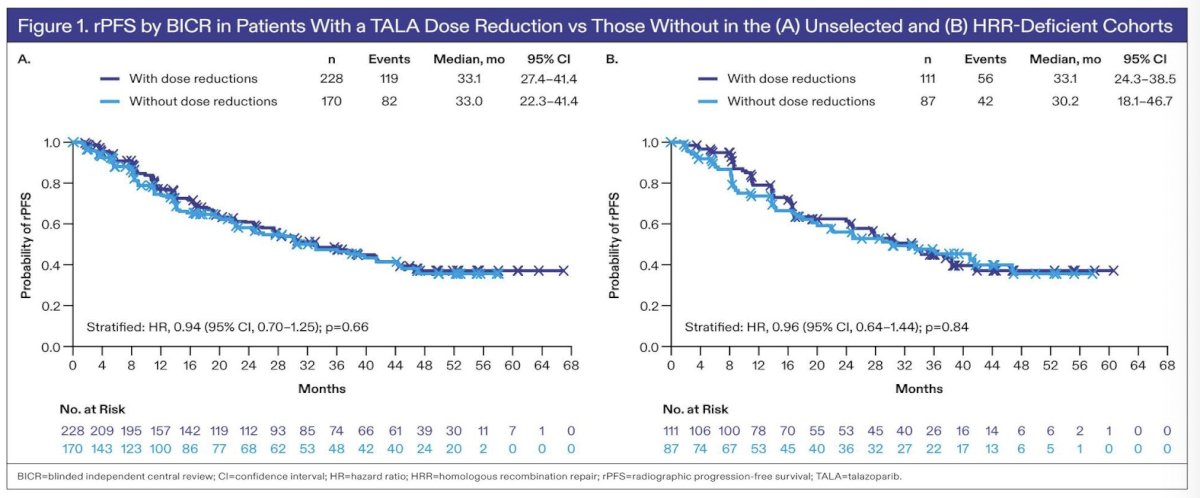
Figure 2 evaluated PSA response rates. PSA response rates remained high and comparable irrespective of dose reduction status. In the unselected cohort, PSA response rates were 86.8% among patients with dose reductions and 83.1% among those without dose reductions (p=0.31). In the HRR-deficient cohort, corresponding PSA response rates were 91.9% and 82.6%, respectively (p=0.06). The duration of soft tissue response was also similar regardless of dose reduction status in both cohorts.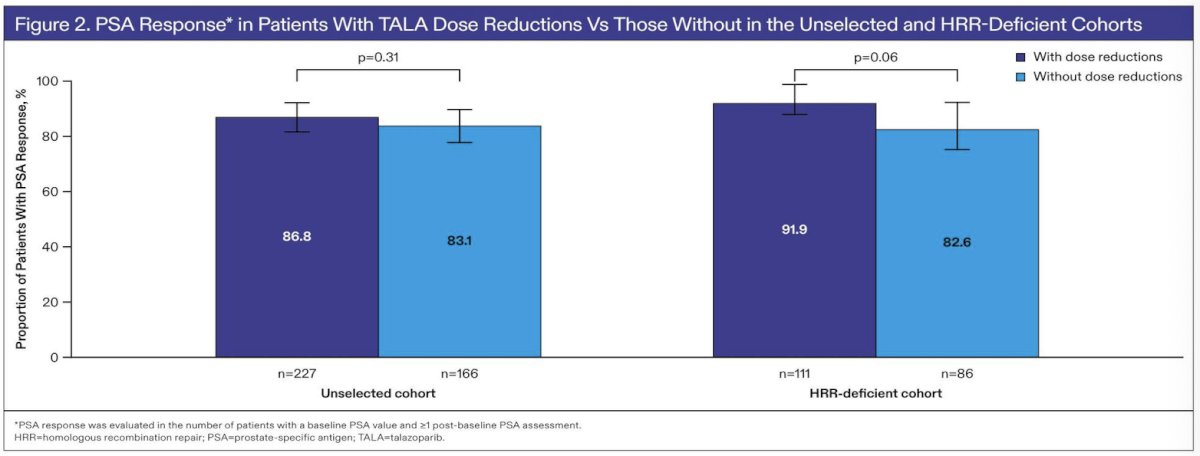
The investigators concluded that older age, Asian ethnicity, lower body weight, mild renal impairment, and baseline anemia were associated with a greater likelihood of TALA dose reductions. Importantly, TALA dose reductions did not adversely affect treatment duration or clinical outcomes, including rPFS, OS, PSA response, or duration of soft tissue response. These findings support proactive toxicity management and appropriate dose modification strategies while maintaining clinical benefit from TALA + ENZA in patients with mCRPC.
Presented by: Ugo De Giorgi, MD, PhD, IRCCS Istituto Romagnolo per lo Studio dei Tumori (IRST), Dino Amadori, Via Piero Maroncelli, 40, 47014 Meldola FC, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: