(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a prostate, testicular, and penile cancers poster session. Dr. Chaochao Liang presented early phase data evaluating HRS-1167 (M9466), a novel PARP1-selective inhibitor, in combination with abiraterone acetate plus prednisone (AA+P) for patients with metastatic castration-resistant prostate cancer (mCRPC).
PARP inhibitor combinations with androgen receptor pathway inhibitors have become an increasingly important treatment strategy in mCRPC, particularly for patients harboring homologous recombination repair (HRR) alterations. While currently approved PARP inhibitors target both PARP1 and PARP2,1-4 selective PARP1 inhibition has emerged as a potentially attractive therapeutic approach aimed at preserving antitumor activity while reducing hematologic toxicity. HRS-1167 is a highly selective PARP1 inhibitor that has previously demonstrated antitumor activity in advanced solid tumors. This phase 1b/2 study evaluated the safety, tolerability, and preliminary efficacy of HRS-1167 combined with AA+P in patients with previously treated HRR-mutated mCRPC.
This was a multicenter, open-label, dose-finding and efficacy expansion study (NCT06689163) conducted in Chinese adult patients with HRR-mutated mCRPC who had received prior therapy. Patients received oral HRS-1167 at either 30 mg daily or 50 mg daily in combination with abiraterone acetate 300 mg daily and prednisone 5 mg twice daily. The primary study objectives were safety and tolerability.
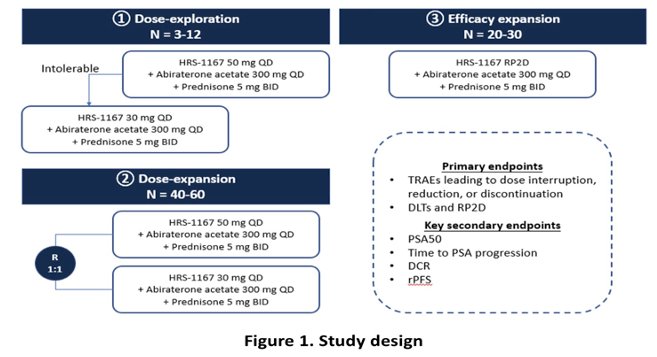
As of the October 31, 2025, data cutoff, 58 patients had been enrolled and treated, including 33 patients in the 30 mg cohort and 25 in the 50 mg cohort. All patients had received prior novel hormonal agent therapy, and 44.8% harbored BRCA mutations. The median follow-up was 3.0 months in the 30 mg cohort and 6.2 months in the 50 mg cohort.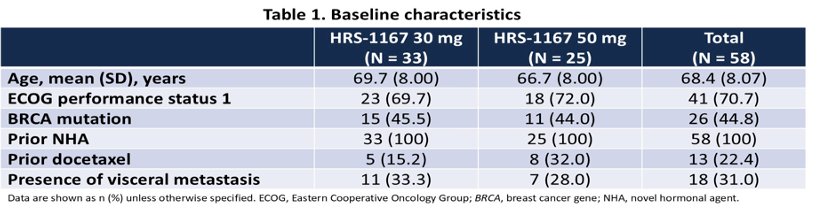
Among efficacy-evaluable patients (n=47), encouraging PSA and clinical activity were observed across both dose levels. PSA50 responses were achieved in 36.4% of patients receiving 30 mg (8/22) and 52% receiving 50 mg (13/25). Confirmed objective response rates (cORR) were 37.5% and 14.3%, while disease control rates (DCR) were 81.8% and 92.0% in the 30 mg and 50 mg cohorts, respectively.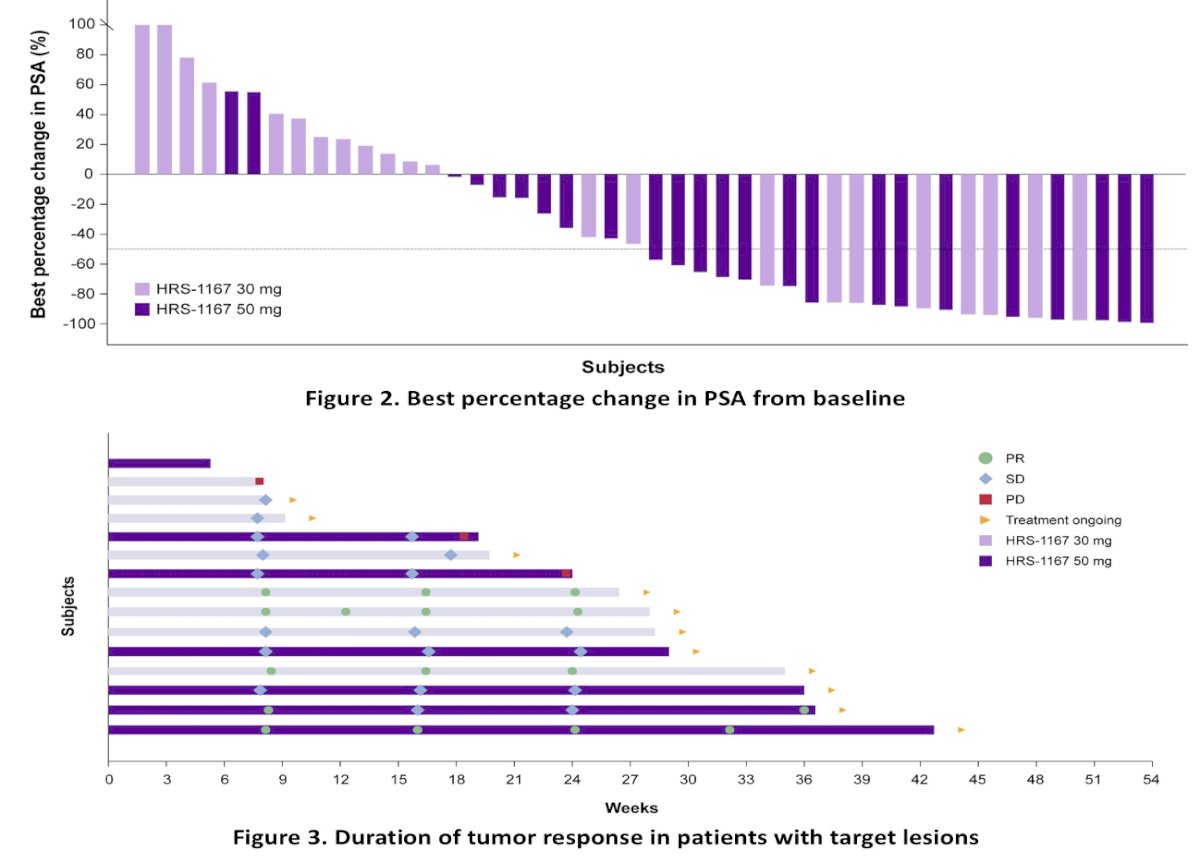
Strong activity was observed among patients with BRCA mutations. In this subgroup, PSA50 response rates reached 100% (6/6) in the 30 mg cohort and 81.8% (9/11) in the 50 mg cohort. Confirmed objective response rates were 100% (2/2) and 33.3% (1/3), respectively, while DCR was 100% across both BRCA-mutated cohorts. The median time to PSA progression was not reached in the 30 mg cohorts and was 6.5 months in both 50 mg cohorts.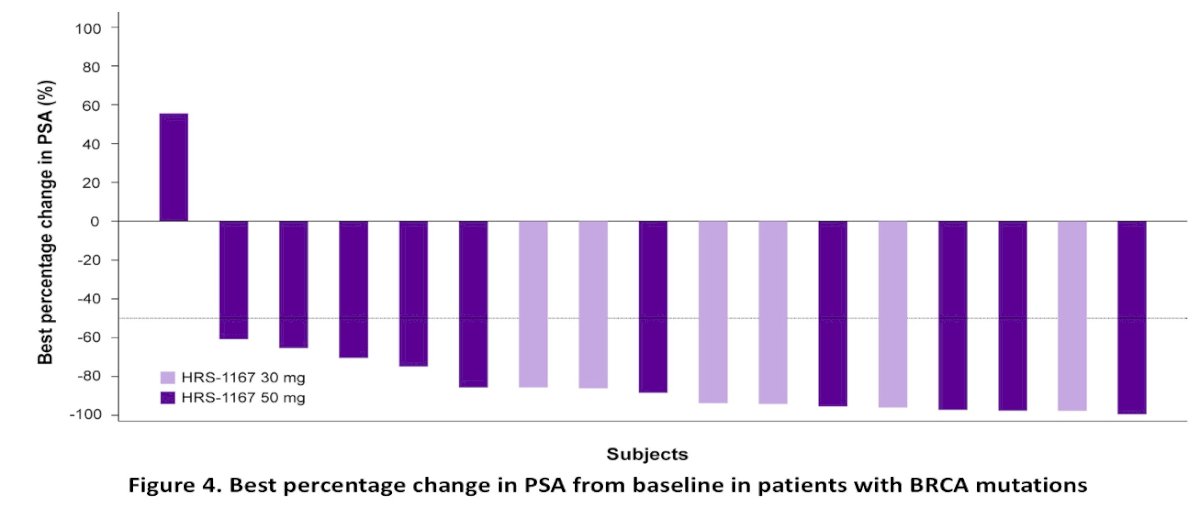
The combination demonstrated a manageable safety profile without new safety signals identified. Treatment-emergent adverse events (TEAEs) occurred in 78.8% of patients receiving 30 mg and 100% receiving 50 mg, with grade ≥3 TEAEs reported in 18.2% and 44%, respectively. Serious TEAEs occurred in 9.1% and 32% of patients. Importantly, no TEAEs leading to death were observed.
The most common grade ≥3 toxicities were hematologic in nature, including anemia (9.1% versus 24%), decreased platelet count (6.1% versus 8%), decreased white blood cell count (0% versus 12%), and decreased neutrophil count (3% versus 8%) in the 30 mg and 50 mg cohorts, respectively.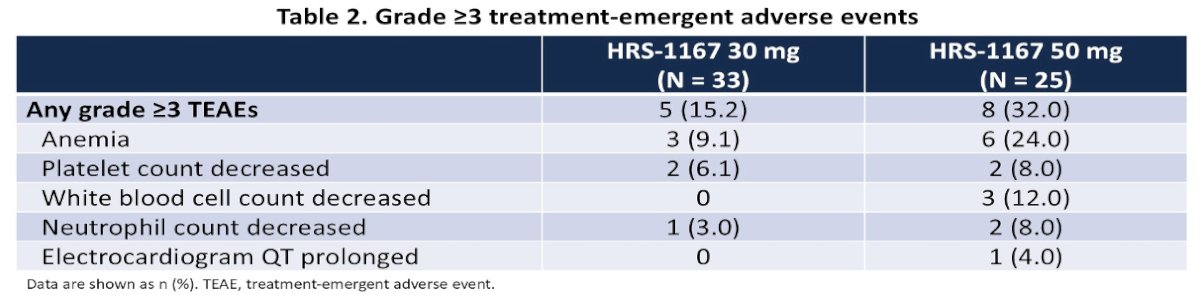
The investigators concluded that HRS-1167 combined with AA+P demonstrated promising preliminary efficacy in patients with mCRPC, particularly among those harboring BRCA mutations, while maintaining an acceptable safety profile without new toxicity concerns.
These findings are clinically relevant because they further support PARP-based combination strategies in HRR-mutated mCRPC while also highlighting the potential therapeutic role of selective PARP1 inhibition. Although follow-up remains short and patient numbers are limited, the high PSA50 and disease control rates observed in BRCA-mutated patients are encouraging. Additional follow-up and larger studies will be important to better define the durability of response, comparative efficacy, and whether selective PARP1 inhibition may offer a differentiated safety profile relative to currently available PARP inhibitors in prostate cancer.
Presented by: Chaochao Liang, The First Affiliated Hospital of Anhui Medical University, Hefei, China
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- U.S. Food and Drug Administration. FDA Approves Olaparib and Rucaparib for Metastatic Castration-Resistant Prostate Cancer. National Cancer Institute Cancer Currents Blog. Published May 27, 2020. Accessed June 1, 2026. National Cancer Institute Cancer Currents Blog
- U.S. Food and Drug Administration. FDA Approves Niraparib and Abiraterone Acetate Plus Prednisone for BRCA-Mutated Metastatic Castration-Resistant Prostate Cancer. Published August 11, 2023. Accessed June 1, 2026. FDA Drug Approval Announcement
- U.S. Food and Drug Administration. FDA Approves Talazoparib With Enzalutamide for HRR Gene-Mutated Metastatic Castration-Resistant Prostate Cancer. Published June 20, 2023. Accessed June 1, 2026. FDA Drug Approval Announcement
- U.S. Food and Drug Administration. FDA Approves Olaparib With Abiraterone and Prednisone (or Prednisolone) for BRCA-Mutated Metastatic Castration-Resistant Prostate Cancer. Published May 31, 2023. Accessed June 1, 2026. FDA Drug Approval Announcement